التشخيص
A diagnosis of invasive ductal carcinoma (IDC) may begin with an exam and a discussion of your symptoms. Sometimes the diagnosis starts when an imaging test, such as a mammogram, finds something concerning in a breast. To confirm whether there is cancer or not, your healthcare professional may recommend a procedure called a biopsy to remove breast tissue for testing. While many tests can spot something in the breast that may be cancer, a biopsy is the only test that can say whether you have invasive ductal carcinoma.
Breast exam
During a breast exam, a healthcare professional looks at the breasts for anything that's not typical. This might include changes in the skin or to the nipple. Then the health professional feels the breasts for lumps. The health professional also feels along the collarbones and around the armpits for lumps.
Mammogram
الحصول على صورة الثدي الشعاعية
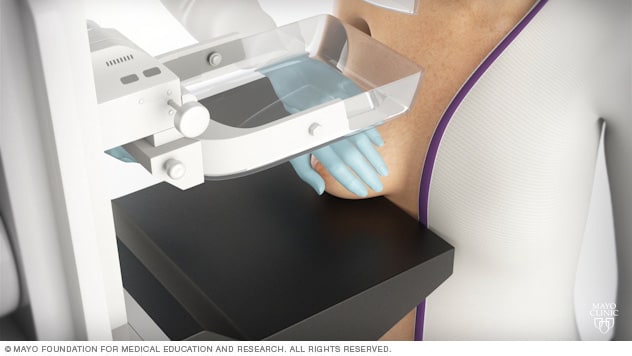
الحصول على صورة الثدي الشعاعية
أثناء صورة الثدي الشعاعية (الماموغرام)، تقفين أمام جهاز الأشعة السينية المصمم لتصوير الثدي الشعاعي. ثم تضع مساعدةٌ فنيةٌ ثديَ المريضة على سطح مستوٍ بعد أن تضبط ارتفاع هذا السطح ليناسب طول المريضة. وبعدها تساعدكِ على ضبط وضعية الرأس والذراع والجذع بطريقة لا تعوق رؤية الثدي.
A mammogram is an X-ray of the breast tissue. Mammograms are commonly used to screen for breast cancer. If a screening mammogram finds something concerning, you might have another mammogram to look at the area more closely. This more-detailed mammogram is called a diagnostic mammogram. It's often used to look closely at both breasts.
On a mammogram, invasive ductal carcinoma typically looks like a growth with irregular borders.
Breast ultrasound
Ultrasound uses sound waves to make pictures of structures inside the body. A breast ultrasound may give your healthcare team more information about a breast lump. For example, an ultrasound might show whether the lump is a solid mass or a fluid-filled cyst. The healthcare team uses this information to decide what tests you might need next.
On a breast ultrasound, invasive ductal carcinoma typically looks like a dark spot with an irregular border. The ultrasound may show thin lines extending from the edge of the cancer.
Breast MRI
تصوير الثدي بالرنين المغناطيسي
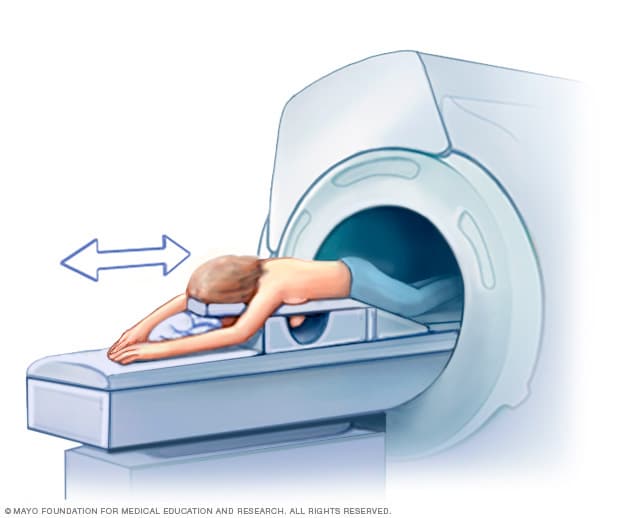
تصوير الثدي بالرنين المغناطيسي
يتضمن تصوير الثدي بالرنين المغناطيسي الاستلقاء على البطن على طاولة فحص مبطنة.
ويُدخل الثديان في تجويف مفرّغ موجود في الطاولة.
يحتوي التجويف على ملفات تستقبل الإشارات من جهاز التصوير بالرنين المغناطيسي.
ثم تنزلق الطاولة إلى الفتحة الكبيرة لهذا الجهاز.
MRI machines use a magnetic field and radio waves to create pictures of the inside of the body. A breast MRI can make more-detailed pictures of the breast. Sometimes this method is used to look closely for any other areas of cancer in the affected breast. It also might be used to look for cancer in the other breast. Before a breast MRI, you usually receive an injection of contrast material. The contrast helps the tissue show up better in the images.
Breast biopsy
الخزعة الداخلية بالإبرة
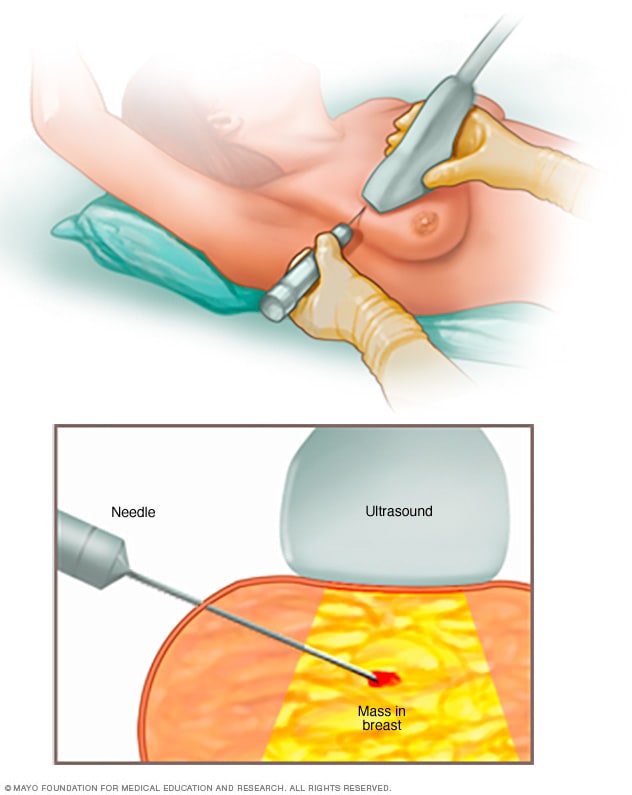
الخزعة الداخلية بالإبرة
عند خزع اللب بالإبرة، يُستخدم أنبوب طويل ومجوف لأخذ عينة من الأنسجة. هنا، تُؤخذ الخزعة من كتلة مشتبه فيها من الثدي. ثم تُرسَل العينة إلى المختبر لفحصها بواسطة أطباء يطلق عليهم خبراء الأمراض. وهم مختصون في فحص الدم وأنسجة الجسم.
A biopsy is a procedure to remove a sample of tissue for testing in a lab. For a breast biopsy, a healthcare professional puts a needle through the skin and into the breast tissue. The health professional guides the needle using images created with X-rays, ultrasound or another type of imaging. Once the needle reaches the right place, the health professional uses the needle to draw out tissue from the breast. A marker may be placed in the spot where the tissue sample was removed. This small metal marker shows up on imaging tests. It helps your healthcare team mark the area of concern.
Lab testing
The tissue sample from a biopsy goes to a lab for testing. Tests can show whether the cells in the sample are cancerous. Other tests give more details about the cells. The testing is done by pathologists. Pathologists are doctors who look for disease in cells, fluids and tissue removed from the body.
Results are often given in a pathology report. The results may show:
- Cell type. The results show whether the cancer cells are ductal cells, lobular cells or other kinds of cells. Invasive ductal carcinoma contains ductal cells.
- Cell grade. The grade of the breast cancer cells is based on how the cells look under a microscope. The grade tells the healthcare team whether the cancer is likely to grow slowly or quickly.
- Hormone receptor status. Most breast cancer cells use the hormones estrogen and progesterone to help them grow. Cells that do this have receptors that help them catch the hormones circulating in the bloodstream. If testing finds receptors for one or both hormones, the cancer is hormone receptor positive. If testing doesn't find receptors, then the cancer is hormone receptor negative.
- HER2 status. Some breast cancer cells use a protein called human epidermal growth factor receptor 2 (HER2) to help them grow. Healthy breast cells make some HER2, but the cancer cells can make a lot more. If tests show the cancer cells have extra copies of the HER2 gene or increased levels of the HER2 protein, the cancer is HER2 positive. If testing doesn't find these, the cancer is HER2 negative.
- Ki-67 score. Ki-67 is a protein that marks how fast the cancer cells divide, also called the proliferation rate. The Ki-67 score goes from 0% to 100%. A higher score suggests a higher rate of dividing cells and faster growth.
The healthcare team uses the results from lab tests to decide on the cancer's stage, understand the prognosis and make a treatment plan.
Staging tests
Once your healthcare team diagnoses invasive ductal carcinoma, you may have other tests to figure out the extent of the cancer. This is called the cancer's stage. Your healthcare team uses your cancer's stage to understand your prognosis.
Complete information about your cancer's stage may not be available until after breast cancer surgery.
Tests and procedures used to stage breast cancer may include:
Not everyone needs all of these tests. Your healthcare team picks the right tests based on your specific situation.
Invasive ductal carcinoma uses the same stages as other types of breast cancer. Breast cancer stages range from 0 to 4. A lower number means the cancer is less advanced and more likely to be cured. As the cancer grows into the breast tissue and gets more advanced, the stages get higher.
للمزيد من المعلومات
Grades
A cancer's grade is a number that tells the healthcare team how different the cancer cells look from healthy cells. The grades of invasive ductal carcinoma (IDC) go from 1 to 3.
To decide on the grade, doctors in the lab, called pathologists, use a microscope to look at the cancer cells from a biopsy. If the cancer cells look similar to healthy cells, then the cancer cells are low grade. Low-grade cancer grows slowly. If the cancer cells look very different from healthy cells, then the cancer cells are high grade. High-grade cancer grows quickly.
The grades of invasive ductal carcinoma include:
- Grade 1. Grade 1 is a low grade. The cancer cells look similar to healthy cells. Grade 1 invasive ductal carcinoma typically grows slowly and has a low risk of spreading. It's sometimes called well-differentiated cancer.
- Grade 2. Grade 2 is an intermediate grade. The cancer cells look a little different from healthy cells. Grade 2 invasive ductal carcinoma grows more quickly than grade 1 cancer. It also has a higher risk of spreading. Sometimes it's called moderately differentiated cancer.
- Grade 3. Grade 3 is a high grade. The cancer cells look very different from healthy cells. Grade 3 invasive ductal carcinoma is considered a fast-growing cancer. It has the highest risk of spreading. Sometimes it's called poorly differentiated cancer.
The grade helps the healthcare team understand the prognosis and make a treatment plan. High-grade cancers are more likely to spread, so they may need more intense treatment. Grade 1 or 2 invasive ductal carcinoma cells are more likely to have hormone receptors and respond to estrogen blocker therapy. Grade 3 cancers are more likely to respond to chemotherapy.
العلاج
Invasive ductal carcinoma (IDC) treatment often involves surgery to remove the cancer. Other treatment options include radiation therapy, chemotherapy, estrogen blocker therapy, targeted therapy and immunotherapy. Most people have more than one treatment.
Invasive ductal carcinoma treatment is similar to treatment for other types of breast cancer. There are no treatments that are specific to invasive ductal carcinoma. Your treatment options depend more on the stage of your cancer, the hormone receptor status and the HER2 status.
Most people with stage 1 or stage 2 invasive ductal carcinoma will have surgery as the first treatment. Most also will have other treatments after surgery, such as radiation, chemotherapy or estrogen blocker therapy. These other treatments kill any cancer cells that might be left after surgery and lower the risk that the cancer will come back.
Sometimes treatment starts with medicines. Your care team might recommend this if you have a stage 3 invasive ductal carcinoma that has grown large or spread to the lymph nodes. Using medicine first may shrink the cancer so that surgery is possible or so that you might consider a less invasive surgery. It also gives your care team a chance to see how the cancer responds to medicines. The response tells the care team about your prognosis and helps them make decisions about the next steps.
For a stage 4 invasive ductal carcinoma that has spread to other parts of the body, treatment uses medicines. Surgery usually isn't used to remove the cancer in the breast if the cancer has spread.
There are many options for breast cancer treatment. You don't have to sort through them on your own. Your healthcare team can help explain your options and work with you to choose a treatment plan that fits your needs and goals. Consider seeking a second opinion from a breast specialist in a breast center or clinic. Some people also find it helpful to talk with breast cancer survivors who have faced similar decisions.
Breast cancer surgery
استئصال الكتلة
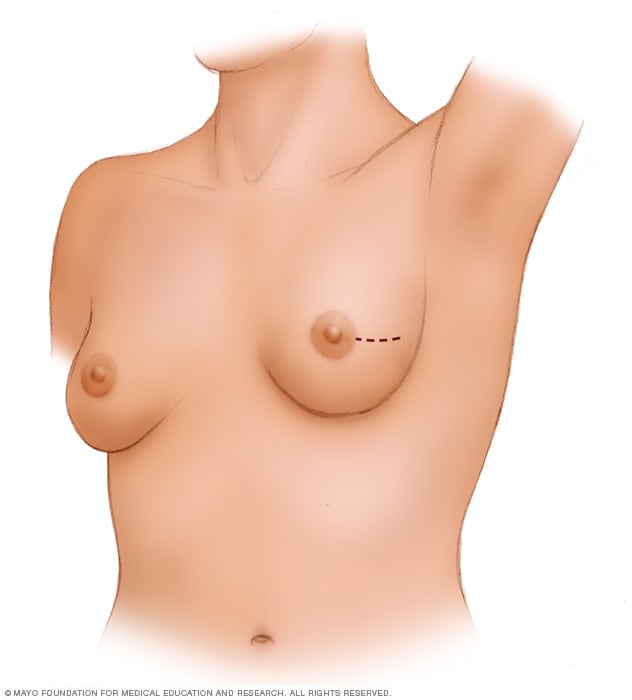
استئصال الكتلة
يتضمن استئصال الكتلة إزالة الورم السرطاني وبعض الأنسجة السليمة المحيطة به.
وتوضح هذه الصورة أحد الأشكال المحتملة للشقوق التي يُمكن إحداثها لتنفيذ هذا الإجراء، غير أن الجرّاح هو من يحدد الطريقة الأفضل حسب حالتك.
استئصال الثدي

استئصال الثدي
في عملية الاستئصال الكامل للثدي، يستأصل الجراح نسيجَ الثدي، والحلمة، والهالة، والجلد. ويسمى هذا الإجراء أيضًا الاستئصالَ البسيط للثدي. وهناك إجراءات أخرى لاستئصال الثدي قد تترك بعض الأجزاء من الثدي، كالجلد أو الحلمة. ويمكن أن تُجرى جراحة لإعادة بناء ثدي جديد حسب اختيار المريضة. ويُمكن إجراؤها بعد استئصال الثدي في العملية نفسها أو في وقت لاحق.
Breast cancer surgery typically involves a procedure to remove the breast cancer and, sometimes, a procedure to remove some nearby lymph nodes. The main surgical procedures used to treat invasive ductal carcinoma include:
- Lumpectomy. A lumpectomy is surgery to remove the breast cancer and some of the healthy tissue around it. It allows you to maintain most of your breast. Other names for this surgery are breast-conserving surgery and wide local excision. Most people have radiation therapy after lumpectomy.
- Mastectomy. A mastectomy is surgery to remove all breast tissue from a breast. Total mastectomy, also called simple mastectomy, removes all of the breast, including the lobules, ducts, fatty tissue and some skin, including the nipple and areola. Other procedures include skin-sparing mastectomy, which leaves the skin, and nipple-sparing mastectomy, which leaves the areola, nipple and skin.
- Lymph node surgery. Lymph node surgery removes nearby lymph nodes to check them for cancer. When breast cancer spreads it most often goes to the lymph nodes under the arm. A sentinel node biopsy removes some of those lymph nodes for testing. An axillary lymph node dissection removes most of the underarm lymph nodes.
For early-stage invasive ductal carcinoma, lumpectomy followed by radiation has the same survival rate as mastectomy. The type of cancer doesn't affect which procedure you should have. The decision depends more on your personal preferences and the details of your cancer. Lumpectomy is preferred for small cancers in people who are willing to have radiation. Lumpectomy is typically used when there is only one small area of cancer in the breast. Mastectomy is preferred for larger cancers or when there are multiple areas of cancer in the breast. Mastectomy might be used in those who don't want or can't have radiation.
You may choose to have breast reconstruction after mastectomy surgery. Breast reconstruction is surgery to restore the shape to the breast. Options might include reconstruction with a breast implant or reconstruction using your own tissue. Consider asking for a referral to a plastic surgeon before your breast cancer surgery.
Radiation therapy
العلاج الإشعاعي
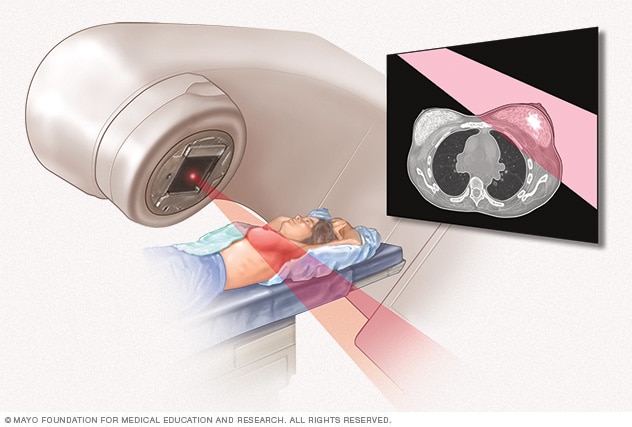
العلاج الإشعاعي
تَستخدم الحزم الإشعاعية الخارجية حزمًا عالية الطاقة لقتل الخلايا السرطانية.
تُوجَّه الحزم الإشعاعية بدقة نحو الورم السرطاني باستخدام جهاز يتحرك حول الجسم.
Radiation therapy treats cancer with powerful energy beams. The energy can come from X-rays, protons or other sources.
Radiation therapy for breast cancer often uses external beam radiation. During this type of radiation therapy, you lie on a table while a machine moves around you. The machine directs radiation to precise points on your body.
Radiation therapy is often used after surgery for invasive ductal carcinoma. It can kill any cancer cells that might be left after surgery. The radiation lowers the risk of the cancer coming back.
Chemotherapy
Chemotherapy treats cancer with strong medicines. Many chemotherapy medicines exist. Chemotherapy for breast cancer often involves a combination of medicines. Most are given through a vein. Some are available in pill form.
Chemotherapy is often used after surgery to treat invasive ductal carcinoma. It can kill any cancer cells that might remain and lower the risk of the cancer coming back.
Sometimes chemotherapy is given before surgery. This may help shrink the cancer so that surgery is possible or so that you might consider a less invasive surgery. It also gives the care team a chance to see how the cancer responds to medicines.
When the cancer spreads to other parts of the body, chemotherapy can help control it. Chemotherapy may relieve symptoms of an advanced cancer, such as pain.
Estrogen blocker therapy
Estrogen blocker therapy treats breast cancer that is sensitive to hormones. This means the cancer cells have proteins called receptors. The receptors bind to the hormones estrogen and progesterone. The cancer grows in response to these hormones. Healthcare professionals call these cancers hormone receptor positive. Most breast cancers, including most invasive ductal carcinomas, are sensitive to hormones.
Estrogen blocker therapy also is called endocrine therapy and hormone therapy for breast cancer.
Estrogen blocker therapy treatments can include:
- Medicines that block or destroy hormone receptors. These medicines are called selective estrogen receptor modulators.
- Medicines that lower hormone production. These medicines are called aromatase inhibitors.
- Surgery or medicines to stop the ovaries from making hormones.
Estrogen blocker therapy often is used after surgery and other treatments. It can lower the risk that the cancer will come back.
If the cancer spreads to other parts of the body, estrogen blocker therapy can help control it.
Targeted therapy
Targeted therapy uses medicines that attack specific chemicals in the cancer cells. By blocking these chemicals, targeted treatments can cause cancer cells to die.
Some treatments target cancer cells that make extra HER2. Breast cancer that makes extra HER2 is called HER2-positive breast cancer. Other targeted therapy medicines attack other proteins in the body that help cancer cells grow. Your cancer cells may be tested to see whether these medicines might help you.
Targeted therapy medicines may be used before surgery to shrink the cancer and make it easier to remove. They also may be used after surgery to lower the risk that the cancer will come back.
Some targeted therapy medicines are used only when the cancer has spread to other parts of the body.
Immunotherapy
Immunotherapy is a treatment with medicine that helps the body's immune system to kill cancer cells. The immune system fights off diseases by attacking germs and other cells that shouldn't be in the body. Cancer cells survive by hiding from the immune system. Immunotherapy helps the immune system cells find and kill the cancer cells.
Immunotherapy might be an option for treating invasive ductal carcinoma that's triple negative. Triple-negative breast cancer means that the cancer cells don't have hormone receptors and don't make extra HER2. This treatment may be used before and after surgery.
للمزيد من المعلومات
التأقلم والدعم
Learning you have invasive ductal carcinoma (IDC) can be unexpected, and it's natural to have questions about what comes next. You may be receiving a lot of information and facing decisions about surgery, radiation and medical treatments. It's common to have a range of feelings that may change from day to day, and it can take time to process everything. As you move forward, here are some ideas that might be helpful.
Learn enough to make decisions about your care
If you'd like to know more about your breast cancer, ask your healthcare team for the details. Write down the type, stage and hormone receptor status. Ask for good sources of information where you can learn more about your treatment options.
Knowing more about your cancer and your options may help you feel more confident when making treatment decisions. Still, some people don't want to know the details of their cancer. If this is how you feel, let your care team know that too.
Talk with other breast cancer survivors
You may find it helpful and encouraging to talk to others who have been diagnosed with breast cancer. Ask your healthcare team about support groups in your area, or contact the American Cancer Society or another cancer organization in your area to find resources. Find support online through Mayo Clinic Connect, a community where you can connect with others for support, practical information and answers to everyday questions.
Find a good listener
Finding someone who is willing to listen to you talk about your hopes and fears can be helpful as you manage a cancer diagnosis. This could be a friend or family member. A counselor, medical social worker or clergy member also may offer helpful guidance and care.
الاستعداد لموعدك
Make an appointment with a doctor or other healthcare professional if you have any symptoms that worry you. If an exam or imaging test shows you might have breast cancer, your healthcare team will likely refer you to a specialist.
Specialists who care for people with breast cancer include:
- Breast health specialists.
- Breast surgeons.
- Doctors who specialize in diagnostic tests, such as mammograms, called radiologists.
- Doctors who specialize in treating cancer, called oncologists.
- Doctors who treat cancer with radiation, called radiation oncologists.
- Genetic counselors.
- Plastic surgeons.
What you can do to prepare
- Write down any symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Write down key personal information, including any major stresses or recent life changes.
- Write down your family history of cancer. Note any family members who have had cancer. Note how each member is related to you, the type of cancer, the age at diagnosis and whether each person survived.
- Make a list of all medicines, vitamins or supplements that you're taking.
- Keep all of your records that relate to your cancer diagnosis and treatment. Organize your records in a binder or folder that you can take to your appointments.
- Consider taking a family member or friend along. Sometimes it can be difficult to absorb all the information provided during an appointment. Someone who accompanies you may remember something that you missed or forgot.
- Write down questions to ask your healthcare professional.
Questions to ask your doctor
Your time with your healthcare professional is limited. Prepare a list of questions so that you can make the most of your time together. List your questions from most important to least important in case time runs out. For breast cancer, some basic questions to ask include:
- What type of breast cancer do I have?
- What is the stage of my cancer?
- Can you explain my pathology report to me? Can I have a copy for my records?
- Do I need any more tests?
- What treatment options are available for me?
- What are the benefits from each treatment you recommend?
- What are the side effects of each treatment option?
- Will treatment cause menopause?
- How will each treatment affect my daily life? Can I continue working?
- Is there one treatment you recommend over the others?
- How do you know that these treatments will benefit me?
- What would you recommend to a friend or family member in my situation?
- How quickly do I need to make a decision about cancer treatment?
- What happens if I don't want cancer treatment?
- What will cancer treatment cost?
- Does my insurance plan cover the tests and treatment you're recommending?
- Should I seek a second opinion? Will my insurance cover it?
- Are there any brochures or other printed material that I can take with me? What websites or books do you recommend?
- Are there any clinical trials or newer treatments that I should consider?
In addition to the questions that you've prepared, don't hesitate to ask other questions you think of during your appointment.
What to expect from your doctor
Be prepared to answer some questions about your symptoms and your health, such as:
- When did you first begin experiencing symptoms?
- Have your symptoms been continuous or occasional?
- How severe are your symptoms?
- Has a mammogram ever detected something concerning?
- Have you ever had a breast biopsy?