التشخيص
If healthcare professionals think you may be having a stroke, things move quickly once you get to the hospital. The first goal is to find out what type of stroke you're having. Health professionals also need to rule out other possible causes of your symptoms, such as a brain tumor or drug reaction.
Tests used to diagnose embolic stroke may include:
- A physical exam and blood tests. A health professional asks about when symptoms started and does several tests. These may include listening to your heart and checking your blood pressure. A neurological exam looks at how a potential stroke is affecting your nervous system. You also may need tests to check how fast your blood clots and whether your blood sugar is too high or low. And you may be tested to see if you have an infection.
- Computerized tomography (CT). A CT scan uses a series of X-rays to create a detailed image of your brain. A CT scan can show bleeding in the brain, an ischemic stroke, a tumor or other conditions. You might have a contrast substance injected into your bloodstream to view the blood vessels in the neck and brain in more detail. This type of test is called a computerized tomography angiography. A test called a CT perfusion scan measures blood flow in the brain.
- Magnetic resonance imaging (MRI). An MRI uses powerful radio waves and a magnetic field to create a detailed view of the brain. The test can detect brain tissue damaged by an ischemic stroke. Sometimes a contrast substance is injected into a blood vessel to view the arteries and veins and highlight blood flow. This test is called magnetic resonance angiography or magnetic resonance venography. A test called a perfusion MRI measures blood flow in the brain.
- Carotid ultrasound. In this test, sound waves create detailed images of the inside of the carotid arteries in the neck. A carotid ultrasound can show buildup of fatty deposits called plaques and blood flow in the carotid arteries.
- Cerebral angiogram. This test is less common, but it provides a detailed view of arteries in the brain and neck. A thin, flexible tube called a catheter is inserted through a small incision, usually in the groin. The tube is guided through the major arteries and into the carotid or vertebral artery in the neck. Then a dye is injected into the blood vessels to make the arteries visible under X-ray imaging.
- Echocardiogram. An echocardiogram uses sound waves to create detailed images of the heart. An echocardiogram can find a source of clots in the heart that may have traveled to the brain and caused a stroke.
- Heart rhythm monitoring. An electrocardiogram (ECG or EKG) can help find atrial fibrillation or another heart rhythm condition that may have caused an embolus. Some people may need longer heart rhythm monitoring after the first evaluation, for example, if the stroke looks embolic but the cause is still not clear. This may include wearing a Holter monitor or an external loop recorder or other device. Or a device, such as an implantable loop recorder, may be implanted under the skin during a minor surgical procedure.
Embolic stroke of undetermined source
Sometimes testing suggests that a stroke was caused by an embolus, but the source is still not clear. You may hear a diagnosis of embolic stroke of undetermined source, also called ESUS.
For a stroke to be identified as ESUS, health professionals must use brain and blood vessel imaging and heart testing to:
- Rule out a small deep type of stroke linked to small blood vessels in the brain.
- Rule out major heart conditions that can cause embolism.
- Find that the artery that supplies the affected brain area has not narrowed by 50% or more.
You also may hear the term cryptogenic stroke. This is a broad term for any ischemic stroke where the cause is not known even after the usual testing.
للمزيد من المعلومات
العلاج
Treatment for embolic stroke needs to happen right away to reduce the chance of brain damage and other complications. The first goal is to restore blood flow to the brain as quickly as possible. This may be done with:
-
Emergency clot busting IV medicine. An IV medicine that can break up a clot has to be given within 4.5 hours from when symptoms began or from when a person was last known to be well. The sooner the medicine is given, the better. Quick treatment improves your chances of survival and may reduce complications.
An IV injection of recombinant tissue plasminogen activator (TPA) is the gold standard treatment for ischemic stroke. An injection of TPA is usually given through a vein in the arm within the first 4.5 hours after stroke symptoms started.
This medicine restores blood flow by dissolving the blood clot causing the stroke. By quickly removing the cause of the stroke, it may help people recover more fully from a stroke. Your healthcare professional considers certain risks, such as potential bleeding in the brain, to decide whether TPA is part of your treatment plan.
-
Removing the clot with a stent retriever, also called mechanical thrombectomy. A device attached to a catheter can directly remove the clot from the blocked blood vessel in the brain. This procedure is especially helpful for people with large clots that can't be completely dissolved with TPA. This procedure often is performed in combination with injected TPA. This procedure may help improve outcomes and reduce long-term disability. It should be done as soon as possible. In some people, it may be used up to 24 hours after the person was last known to be well.
The time window when these procedures can be considered has been expanding due to newer imaging technology. Perfusion imaging tests done with CT or MRI help decide if someone may benefit from thrombectomy. In some people, it may be used up to 24 hours after the person was last known to be well.
Other treatments
Your health professionals may suggest other treatments depending on the cause of the embolic stroke. These treatments may help lower the risk of having another stroke.
- Carotid endarterectomy. Carotid arteries are the blood vessels that run along each side of the neck, supplying the brain with blood. This surgery removes the plaque blocking a carotid artery and may reduce the risk of another stroke. A carotid endarterectomy also involves risks, especially for people with heart disease or other medical conditions.
- Angioplasty and stents. In an angioplasty, a surgeon threads a catheter to the carotid arteries through an artery in the groin. A balloon is then inflated to expand the narrowed artery. Then a stent can be inserted to support the opened artery.
- Medicines and lifestyle changes that help prevent stroke. After the emergency phase, medicines and lifestyle changes to prevent another stroke may be recommended. These can differ depending on what led to the embolic stroke. Some people need antiplatelet or anticoagulant medicines and lifestyle changes that help reduce the risk of clots. Others may need medicines and lifestyle changes to manage conditions, such as high blood pressure, that raise stroke risk.
- Left atrial appendage closure. This procedure may be an option for some people with atrial fibrillation who can't take blood thinners due to bleeding risks. The procedure closes a small sac in the left upper heart chamber. This sac is called an appendage and is where most clots related to atrial fibrillation form. During the procedure a doctor gently guides a closure device through a catheter to the sac. Once the device is in place, the catheter is taken out. The device stays in permanently.
- Patent foramen ovale (PFO) closure. If you have an opening in the heart called a PFO and have had a stroke suspected to be caused by it, you may need a procedure to close the hole. The procedure may be done by inserting a plug into the hole through a thin, flexible tube inserted into the groin and guided to the heart. Or it may be closed with stitches during surgery done through a small incision, sometimes using robotic techniques. PFOs are common. So in most people with a PFO and a stroke, another cause of the stroke is found. Those people do not need the PFO closed.
For fat embolism, treatment is mainly to reduce symptoms and offer supportive care, such as managing blood pressure or using a ventilator to help with breathing.
For air embolism, treatment often includes short-term high-flow oxygen and hyperbaric oxygen therapy. These treatments may improve outcomes if given early after the air embolism.
Stroke recovery and rehabilitation
اتصالات نصف الكرة الدماغية
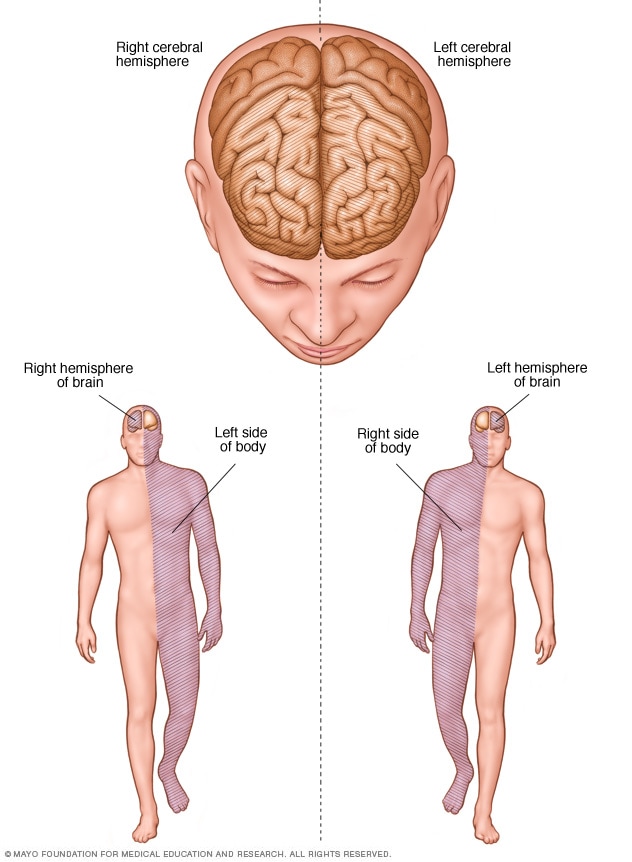
اتصالات نصف الكرة الدماغية
After emergency treatment, you're closely monitored for at least a day. After that, stroke care focuses on helping you recover as much function as possible and to return to independent living. The impact of the stroke depends on the area of the brain involved and the amount of tissue damaged.
If the stroke affected the right side of the brain, movement and feeling on the left side of your body may be affected. If the stroke damaged the left side of the brain, movement and feeling on the right side of your body may be affected. Brain damage to the left side of the brain also may cause speech and language disorders.
Most people who have had a stroke and have remaining symptoms go to a rehabilitation program. Your healthcare professional can recommend the therapy program that is right for you. A program is recommended based on your age, overall health and degree of disability from the stroke. Your lifestyle, interests, priorities and whether you have help from family members or caregivers are considered.
Rehabilitation may begin before you leave the hospital. After discharge, you might continue the program in a rehabilitation unit of the same hospital. Or you may go to another rehabilitation unit or to a skilled nursing facility as an outpatient. You also might have rehabilitation at home.
Every person's stroke recovery is different. Depending on your condition, your treatment team may include a doctor trained in brain conditions, known as a neurologist, a rehabilitation doctor, known as a physiatrist, a rehabilitation nurse, a dietitian, a physical therapist, an occupational therapist, a recreational therapist, a speech pathologist, a social worker or case manager, a psychologist or psychiatrist, or a chaplain.

تشكل معالجة النطق في كثير من الأحيان جزءًا من التأهيل بعد السكتة الدماغية.
للمزيد من المعلومات
Prognosis
Embolic stroke is serious. It can cause disability and can be deadly. Quick treatment improves the chances of survival and may reduce complications. After embolic stroke, some people recover well. Others have lasting disability or need help with daily activities. Recovery depends on a number of factors, including:
- How much of the brain was affected.
- Which part of the brain was affected.
- How quickly treatment began.
Brain damage from an embolic stroke cannot always be fully reversed. Recovery is possible, and some people regain meaningful function. But many do not return to full independence. About half of those who survive more than six months after a stroke need help with at least one daily living activity.
The risk of another embolic stroke is an important part of prognosis. Some causes of embolic stroke carry a higher risk of another stroke than do others. For example, major heart-related embolic sources are linked with a high risk of recurrence.
Ongoing care after embolic stroke is important because treatment and risk reduction can help lower the chance of another stroke and may improve long-term outlook.
التأقلم والدعم
An embolic stroke is a life-changing event that can affect your emotional well-being as much as your physical function. Some people may feel frustrated, depressed or notice mood changes. Some people may have less interest in sex after an embolic stroke.
Maintaining your self-esteem, connections to others and interest in the world are essential parts of your recovery. Several strategies may help you and your caregivers, including:
- Don't be hard on yourself. Physical and emotional recovery involves tough work and takes time. Celebrate your progress. Allow time for rest.
- Join a support group. Meeting with others recovering from a stroke lets you get out and share experiences. You also can exchange information and build new friendships.
- Let friends and family know what you need. People may want to help, but they may not know what to do. Tell them how they can help. For example, ask them to bring over a meal and stay to eat with you and talk. Or ask them to attend social events or religious activities with you.
Communication challenges
If the embolic stroke affected speech and language, these tips may help you and your caregivers cope.
- Practice. Try to have a conversation at least once a day. It can help you learn what works best for you. It also can help you feel connected and rebuild your confidence.
- Relax and take your time. Talking may be easiest and most enjoyable in a relaxing situation when you're not rushed. Some people who have had a stroke find that after dinner is a good time for conversation.
- Say it your way. When you're recovering from a stroke, you may need to use fewer words. Rely on gestures or use your tone of voice to communicate.
- Use props and communication aids. You may find it helpful to use cue cards to communicate. Cue cards can include words used often. Or they can include pictures of close friends and family members, a favorite television show, the bathroom, or other wants and needs.
الاستعداد لموعدك
A stroke in progress is usually diagnosed in a hospital. If you're having a stroke, your immediate care focuses on reducing brain damage. If you haven't had a stroke but you're worried about your risk, talk to your healthcare professional at your next appointment.
What to expect from your doctor
In the emergency room, you may see an emergency medicine specialist or a doctor trained in brain conditions, known as a neurologist. Nurses and medical technicians also are likely to be involved in your care.
Your emergency team's first priority is to stabilize your symptoms and overall medical condition. Then the team decides whether you're having a stroke. Healthcare professionals try to find the cause of the stroke to choose a treatment plan for you.
If you're seeking medical advice during a scheduled appointment, your healthcare professional considers your risk factors for stroke and heart disease. Your health professional can offer advice on how to lower your risk. This may include lifestyle strategies, stopping smoking or not using illicit drugs. Your healthcare professional also may consider if you need medicines to control high blood pressure, cholesterol and other stroke risk factors.