If you're pregnant, you might wonder what exactly the placenta is, what it does and what might affect it. Here's what you need to know about this important organ.
What does the placenta do?
The placenta is an organ that forms in the womb, also called the uterus, during pregnancy. The placenta is connected to a developing baby by a tubelike structure called the umbilical cord. Through the umbilical cord, the placenta provides oxygen and nutrients to a developing baby. It also removes waste from the baby's blood.
The placenta is attached to the wall of the uterus. Most often, it attaches to the top, side, front or back of the uterus. Rarely, it might attach in the lower area of the uterus. When this happens, the placenta may block the passage that connects the uterus to the vagina, called the cervix. If the placenta is near the opening of the cervix, it's known as a low-lying placenta. If it partly or totally covers the opening of the cervix, it causes a condition called placenta previa.
What affects the health of the placenta?
Various factors can affect the health of the placenta, including:
- Age of the pregnant person. Some conditions that affect the placenta are more common in older people, especially after age 40.
- Water breaking before labor. During pregnancy, the developing baby is surrounded and cushioned by a fluid-filled layer of tissue called the amniotic sac. If the sac leaks or breaks before labor starts, it's known as the water breaking. This raises the risk of problems with the placenta.
- High blood pressure. This condition can cause less blood to reach the placenta.
- Being pregnant with twins or other multiples. Being pregnant with more than one baby might raise the risk of some conditions related to the placenta.
- Blood-clotting conditions. Typically, blood hardens into a clump to help control bleeding from cuts. This process is called clotting. Sometimes, blood clots form inside the body and lead to medical problems. Conditions that cause blood to clot too little or too much raise the risk of some conditions related to the placenta.
- Past surgery on the uterus. C-section, surgery to remove tumors called fibroids and other uterine surgeries raise the risk of some conditions that affect the placenta.
- Previous conditions that affected the placenta. The risk of having medical issues with the placenta might be higher if you had problems with the placenta during a past pregnancy.
- Substance use. Some conditions that can affect the placenta are more common in pregnant people who smoke or use cocaine.
- Injury to the stomach area. A blow to the stomach area makes the placenta more likely to separate from the uterus too soon. Risk factors include trauma from a car accident or a serious fall.
What are the most common conditions and concerns?
Conditions that can affect the placenta include:
- Placental abruption. This is when the placenta partly or completely peels away from the inner wall of the uterus before delivery. With placental abruption, the developing baby might not get enough oxygen and nutrients. The pregnant person might have back or stomach pain and bleeding from the vagina. Placental abruption can lead to an emergency in which a baby needs to be delivered early.
-
Placenta previa. This condition happens when the placenta partly or totally covers the cervix. Placenta previa is more common early in pregnancy. It might get better on its own as the uterus grows.
Placenta previa can cause serious vaginal bleeding during pregnancy or delivery. Treatment depends on various factors. They include the amount of bleeding, whether bleeding stops, how far along the pregnancy is and the placenta's position. If placenta previa continues late into the pregnancy, a healthcare professional likely will recommend a C-section.
-
Placenta accreta. Most often, the placenta separates from the wall of the uterus after childbirth. With placenta accreta, part or all of the placenta stays firmly attached to the uterus. This condition happens when the blood vessels and other parts of the placenta grow into the uterine wall. This can cause serious blood loss during delivery.
Sometimes, the placenta invades well into the muscles of the uterus or grows through the uterine wall. If this happens, a healthcare professional likely will recommend a C-section followed by surgery to remove the uterus. This is called a C-hysterectomy.
- Retained placenta. With a vaginal birth, the placenta most often is delivered soon after the baby. But if the placenta isn't delivered within 30 minutes after childbirth, it's known as a retained placenta. A retained placenta might happen because the placenta becomes trapped behind a partially closed cervix. Or it might happen because the placenta is still attached to the uterine wall.
Without treatment, a retained placenta can cause a serious infection or life-threatening blood loss. Treatment may include medicine to help deliver the placenta or a procedure to remove the placenta.
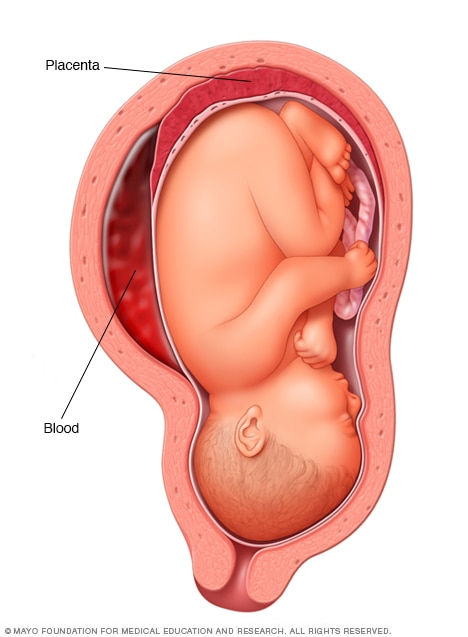
Placental abruption
The placenta is a structure that develops in the uterus during pregnancy. Placental abruption occurs when the placenta separates from the inner wall of the uterus before birth. Placental abruption can deprive the baby of oxygen and nutrients and cause heavy bleeding in the pregnant person. In some people, early delivery is needed.
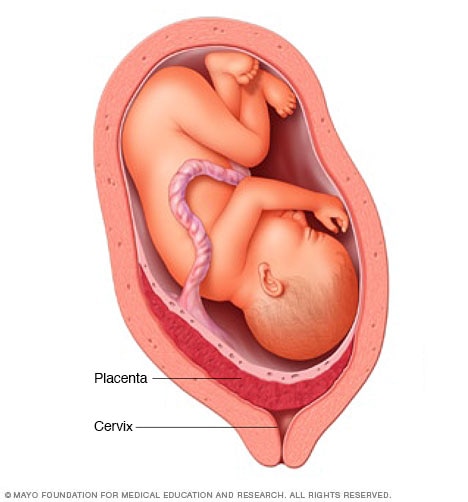
Placenta previa
The placenta is a structure that develops in the uterus during pregnancy. In most pregnancies, the placenta is located at the top or side of the uterus. In placenta previa, the placenta is located low in the uterus. The placenta might partially or completely cover the cervix, as shown here. Placenta previa can cause severe bleeding in a pregnant person before or during delivery. A C-section often is needed.
What are symptoms of trouble with the placenta?
Call your healthcare professional if you have any of the following symptoms during pregnancy:
- Bleeding from the vagina, especially if it's heavy.
- Pain in the stomach area, also called the abdomen.
- Back pain.
- Tightening and relaxing of the muscles in the uterus, also called uterine contractions.
What can I do to lower my risk of conditions that affect the placenta?
Most medical issues related to the placenta can't be prevented directly. But you can take steps to boost your chances for a healthy pregnancy:
- Go to all of your routine pregnancy checkups.
- Work with your healthcare professional to manage any health conditions, such as high blood pressure.
- Don't smoke or use drugs. If you need help quitting, talk with your health care professional.
- If you're thinking about getting a C-section, ask your healthcare professional about the risks.
If you had a condition that affected the placenta during a past pregnancy and you're planning another pregnancy, talk with your healthcare professional. Ask about ways to lower the risk of getting that condition again. Also tell your healthcare professional if you've had surgery on your uterus.
How is the placenta delivered?
If you deliver your baby through your vagina, you'll also deliver the placenta that way shortly afterward. This is known as the third stage of labor.
After you give birth, you keep having mild contractions. Your healthcare professional might give you a shot of medicine called oxytocin (Pitocin). This helps you keep having contractions. It also lessens bleeding after you deliver your baby. Your healthcare professional also might massage your lower abdomen. This encourages the uterus to contract and release the placenta through the vagina. You might be asked to push to deliver the placenta.
If you have a C-section, your healthcare professional removes the placenta from your uterus during that procedure.
After it's delivered, your health care professional checks the placenta to make sure it's intact. Any pieces left behind need to be removed from the uterus to prevent bleeding and infection. If you're interested, ask to see the placenta. In some cultures, families bury the placenta in a special place.
If you have questions about the placenta during pregnancy, talk with a member of your healthcare team. Your healthcare professional can help you better understand the placenta's role in pregnancy.
Mayo Clinic's Ultimate Guide to Pregnancy
This guide offers research-backed advice to help you and your baby experience a healthy pregnancy, written by some of the world's leading medical experts.