概述
大肠,包括结肠、直肠和肛门
大肠,包括结肠、直肠和肛门
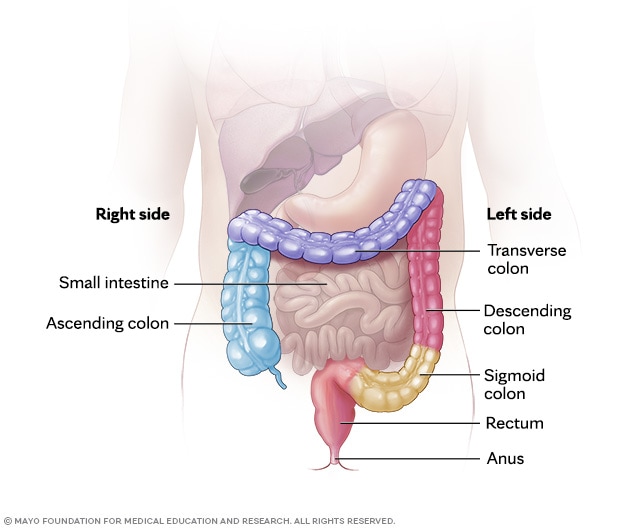
完整的大肠包括升结肠、横结肠、降结肠、乙状结肠、直肠和肛门。
结肠切除术是切除全部或部分结肠的外科类手术。结肠属于大肠的一部分,是消化道末端的长管状器官。为了治疗或预防影响结肠的疾病和状况,例如癌症、克罗恩病、溃疡性结肠炎或憩室炎,或许有必要进行结肠切除术。结肠切除术也被称为结肠切除。
结肠切除术通常需要进行结肠造口术或回肠造口术等造口术。造口术把消化系统的剩余部分重新连接在一起,让身体能够把废物排出体外。
类型
结肠切除术有多种类型。其名称取决于结肠的哪一部分被切除。外科医生根据疾病所在部位选择手术类型。最常见的类型包括:
- 右半结肠切除术。 该手术切除升结肠,有时包括小肠末段和横结肠起始段。它是最常见的结肠切除术类型。
- 左半结肠切除术。 该手术切除结肠的左侧部分。这通常包括从横结肠中部向下至降结肠的结肠部分,往往止于直肠上段。
- 乙状结肠切除术。 该手术切除乙状结肠。这是连接结肠和直肠的弯曲部分。
- 节段性切除术。 该手术仅切除结肠的一小段病变部分。然后将两个健康的端部重新缝合或钉在一起,恢复肠道连贯。
- 低位前切除术。 该手术切除直肠的上部,通常用于治疗直肠癌,并期望保留肛门和肠道功能。
- 经腹会阴直肠切除术(APR)。 该手术切除乙状结肠、直肠和肛门。由于肛门被切除,因此需要做一个永久性结肠造口,让粪便能够排出体外。
- 结肠全切除术。 该手术切除整个结肠。然后将小肠与直肠相连,从而继续通过肛门排便。
- 结肠直肠切除术。 该手术同时切除结肠和直肠。在许多情况下,会将小肠的末端经腹壁引出,形成回肠造口,以让身体将废物排入造口袋。有时,外科医生也许会用小肠制作一个贮袋(而不是做一个永久性回肠造口),并将贮袋连接到肛门,使粪便能够照常通过肛门排出。该手术被称为回肠肛门吻合术(J 型贮袋术)。
目的
结肠切除术用于治疗和预防影响结肠的疾病和状况,例如:
- 无法控制的出血。 结肠严重出血也许需要手术切除受影响的结肠部分。
- 肠梗阻。 结肠梗阻是紧急医疗状况,也许需要切除全部或部分结肠,具体取决于病情。
- 结肠癌。 如果您患有结肠癌,手术切除癌变部位及周边组织也许是治愈疾病或控制疾病的最佳机会。手术还可能有助于预防出血、梗阻或结肠穿孔等问题,癌变部位不断增大时便可能引发这些状况。早期癌症也许只需通过结肠切除术切除一小部分结肠。晚期癌症也许需要切除更多的结肠。
- 克罗恩病。 如果药物对您没有帮助,切除受影响的结肠部分也许会暂时缓解症状。如果在结肠镜检查(查看结肠的检查)中发现癌前病变,结肠切除术也许亦是一个选项。
- 溃疡性结肠炎。 如果药物无法帮助控制症状,医生也许会建议进行结肠全切除术或结肠直肠切除术。如果在结肠镜检查中发现癌前病变,医生也可能建议进行结肠直肠切除术。
- 憩室炎。 如果憩室炎复发或出现憩室炎并发症,医生也许会建议手术切除受影响的结肠部分。并发症可能包括感染、梗阻、结肠穿孔或瘘管(结肠与邻近器官之间形成的通道)。
- 预防性手术。 如果由于形成多个癌前结肠息肉而导致患结肠癌的风险极高,也许可选择进行结肠全切除术以预防未来患上癌症。对于存在可增加患结肠癌风险的遗传性基因状况(如家族性腺瘤性息肉病或林奇综合征)的人群,结肠切除术也许是一个选项。
与医护团队讨论您的治疗选项。在某些情况下,您也许可在多种类型的结肠切除术间做出选择。医护团队会讨论各种手术的益处和风险。
风险
结肠切除术有引起严重并发症的风险。并发症风险取决于总体健康状况、结肠切除术的类型以及外科医生进行该手术的方式。
总体而言,结肠切除术的并发症包括:
- 出血。
- 腿部血凝块(深静脉血栓)和肺部血凝块(肺栓塞)。
- 感染。
- 结肠附近器官(例如膀胱和小肠)的损伤。
- 重新缝合消化系统的其余部分的缝合处撕裂的风险。
在接受结肠切除术后,将留院观察一段时间,以恢复消化系统健康。医护团队将监测手术引起的并发症的体征。
如何进行准备
在结肠手术前的几天里,医护团队可能会要求您:
- 停止服用某些药物。 某些药物可能会增加手术期间出现并发症的风险,因此医护团队也许会要求您在手术前停止服用这些药物。
- 手术前禁食。 医护团队将为您提供具体说明。您可能需要在手术前几小时到一天内停止进食和饮水。
- 喝下清肠的溶液。 医生也许会为您开具泻药溶液,您可在家将其与水混合,并按照说明在几小时内将该溶液喝完。该溶液会导致腹泻,帮助排空结肠。医护团队也许还会建议使用灌肠剂。
- 服用抗生素。 在某些情况下,医生也许会开具抗生素,以杀死结肠内天然存在的细菌并帮助预防感染。
并非所有结肠切除术都能进行术前准备。例如,如果您因肠梗阻或肠穿孔而需要进行急诊结肠切除术,则可能来不及做术前准备。
为您的住院做计划
在结肠切除术后,您需要至少住院几天,具体取决于您的情况。安排他人替您承担您在家庭和工作中的职责。
事先考虑好您在医院康复期间要携带哪些物品。您可能需要带的物品包括:
- 睡袍和拖鞋。
- 洗漱用品,例如牙刷和牙膏,以及剃须用品(如需要)。
- 舒适的衣物,在出院回家时穿。
- 消磨时间的活动,例如书籍、杂志或游戏。
- 您在家使用的任何医疗器械(如治疗睡眠呼吸暂停的 CPAP 机器)。
可能出现的情况
在结肠切除术期间
右半结肠切除术
右半结肠切除术
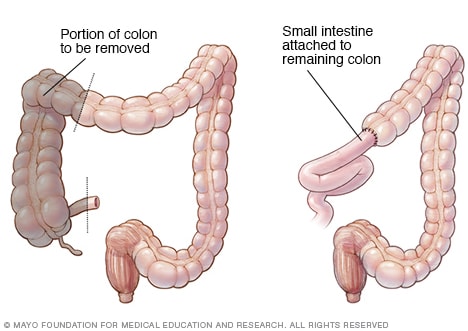
A colectomy procedure to remove one side of the colon is called hemicolectomy. A right hemicolectomy, as shown here, involves removing the right side of the colon and attaching the small intestine to the remaining portion of the colon.
左半结肠切除术
左半结肠切除术
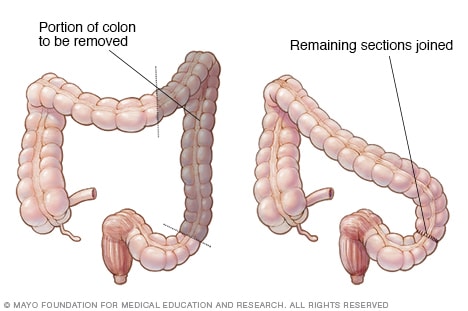
A colectomy procedure to remove one side of the colon is called hemicolectomy. A left hemicolectomy, as shown here, involves removing the left side of the colon and attaching the remaining parts of the colon.
结肠造口术
结肠造口术
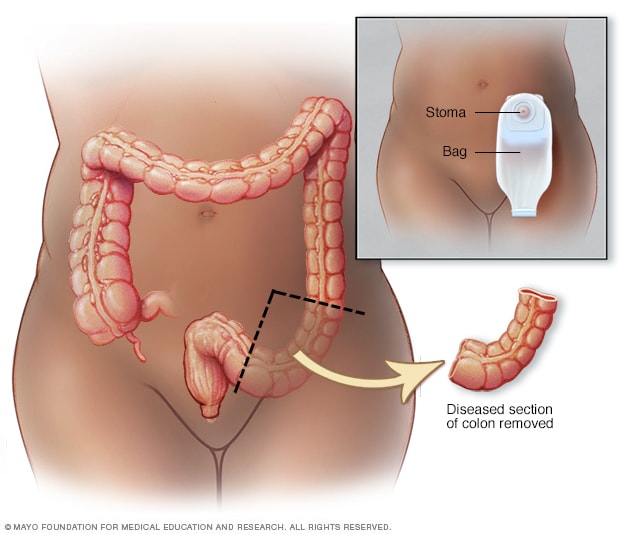
在结肠造口术中,会在腹部做一个开口(称为造口)。将一段结肠从造口拉出并与体外造口袋连接。然后,粪便就可通过造口排入造口袋。
回肠肛管吻合术

回肠肛管吻合术
After proctocolectomy to remove your colon and your rectum, your surgeon may connect your small intestine to your anus (ileoanal anastomosis). This allows you to expel waste normally, though you'll likely have several watery bowel movements daily.
手术当天,医护团队会将您带到准备室。您将接受血压和呼吸监测。您可能会通过手臂静脉接受抗生素药物。
然后,您将被带到手术室,并在手术台上调整好姿势。医务人员会对您施用全身麻醉药物,让您进入类似睡眠的状态,使您在手术过程中不会有任何意识。
然后,手术团队将继续进行结肠切除术。结肠手术可能有两种方式:
手术的类型取决于您的状况和外科医生的专业技能。腹腔镜结肠切除术可减轻术后疼痛并缩短恢复时间。但并不是每个人都适合接受此手术。此外,在某些情况下,即便初始采用腹腔镜结肠切除术,但术中的某些情况也可能迫使手术团队转为开放式结肠切除术。
在修复或切除结肠后,外科医生会重新连接消化系统,以使身体能够排出废物。治疗方案可能包括:
- 重新连接结肠的剩余部分。 外科医生也许会将结肠的健康端部缝合在一起,或者将小肠连接到直肠。这被称为吻合术,让粪便能够照常排出体外。
- 将肠道连接到腹部造口。 如果无法安全地重新连接结肠或直肠,外科医生也许会在腹壁上做一个小开口(称为造口)。废物通过造口排出体外,进入体外佩戴的一个造口袋中。这个程序被称为造口术。结肠造口术和回肠造口术是经常与结肠切除术一起进行的造口术。结肠造口术和回肠造口术可能是临时性的,也可能是永久性的,具体取决于您的状况。
- 连接小肠和肛门。 通过结肠直肠切除术同时切除结肠和直肠后,外科医生也许会用一部分小肠做成一个与肛门连接的贮袋。这被称为回肠肛门吻合术(J 型贮袋术)。J 型贮袋术使您能够以平常方式通过肛门排出废物,但您每天可能会有几次水样便。这种状况通常会随着时间的推移而改善。
外科医生会在手术前与您讨论治疗选项。
结肠切除术后
手术结束后,您会被带到恢复室,在麻醉消退期间接受监护。然后,医护团队会将您送去病房继续康复。
您在肠道功能恢复前需要一直住院,这通常需要几天时间。在这段时间,医护团队会监测疼痛、肠道功能和任何并发症的体征,直到您出院,在家中继续康复之旅。
在接下来几天和几周的恢复期内,大多数患者需要注意以下事项:
- 疼痛管理。 切口部位疼痛是典型状况。需使用药物来控制疼痛。
- 活动。 由于活动有助于预防血凝块和感染性肺炎,因此很可能鼓励您尽快开始活动和行走。大多数患者会在 1 至 2 周内慢慢恢复正常活动。这些活动包括工作、驾驶、淋浴和爬楼梯。
- 肠道功能。 通常需要 3 至 4 天肠道才会开始恢复工作,使您能够排气或排便,并开始照常进食。起初,排便可能会更频繁或更稀薄,但这种状况通常会随着结肠的适应而改善。
- 饮食。 通常在手术后不久开始摄入清流质饮食,然后逐渐添加固体食物。您一开始可能需要避免高脂肪或高纤维食物,尤其是出现腹泻或痉挛时更应如此。
- 疲劳。 持续几周感到虚弱或疲劳是常见状况。身体在大手术后需要时间来恢复力量。
- 切口和伤口护理。 手术部位需要保持清洁,并观察是否出现发红、渗液、肿胀或发热,这些可能是感染的体征。
- 造口护理。 如果您的手术需要通过结肠造口术或回肠造口术来将肠道连至腹部外侧,造口护士会向您讲解如何护理造口。护士会向您说明如何更换收集废物的造口袋。
结果
结肠切除术后,需要几周时间在家康复。一开始您可能感到虚弱,但最终您的体力会恢复。询问医护团队何时能得知该医疗程序的结果。
结肠切除术后的治疗结果主要取决于所治疗的基础病及其严重程度。对许多患者而言,结肠切除术能预防危险的并发症或切除癌变部位,从而保护甚至延长生命。
如果是为了治疗结肠癌而做手术,您需要定期接受结肠镜和影像学随访检查。这有助于尽早发现复发或新发癌症。
Oct. 07, 2025