诊断
肝活检

肝活检
肝活组织检查是指取出少量肝组织样本进行实验室检测。肝活组织检查通常采用一根细针穿过皮肤进入肝脏进行取样。
威尔逊氏症可能很难诊断,因为症状与其他肝病(如肝炎)的症状相似。而且,症状是随时间推移而缓慢出现。逐渐发生的行为变化可能尤其难以与威尔逊氏症相联系。
诊断标准
医务人员会根据症状、实验室检测结果以及影像学或基因检测结果来诊断威尔逊氏症。结构化的评分工具,例如莱比锡诊断标准,可以帮助医务人员结合这些症状和检测结果来确诊或排除威尔逊氏症。该工具根据症状和检测结果进行评分。例如,莱比锡评分达到 4 分或更高,则患有威尔逊氏症的可能性很高。
检查和医疗程序可能包括:
血液和尿液检测
血液检测可以显示肝脏功能状况,并检测铜蓝蛋白(一种与血液中的铜结合的蛋白质)水平。血液检测还可以测定血液中的铜含量。医务人员还可能给您测量 24 小时经尿液排出的铜量。
- 铜蓝蛋白。 该检测用于测定这种与血液中的铜结合的蛋白质的含量。威尔逊氏症患者的铜蓝蛋白水平通常偏低。被视为低数值的具体标准因实验室而异,但低于 20 毫克/升(mg/dL)或 0.2 克/升(g/L)通常属于偏低。铜蓝蛋白之所以水平偏低,是因为导致威尔逊氏症的 ATP7B 基因突变会阻碍铜与其正常结合。有些威尔逊氏症患者的铜蓝蛋白水平并不会降低。而且,即使未患威尔逊氏症,也可能出现铜蓝蛋白水平偏低的情况。例如,由其他因素引起的肝病也可能导致铜蓝蛋白水平降低。
- 血清铜。 这项检测可测定血液中的铜水平。该检测本身并不用于诊断威尔逊氏症。在威尔逊氏症患者中,铜蓝蛋白水平较低,因此血清铜总水平通常也偏低。但是,游离铜(未与铜蓝蛋白结合的铜)的水平通常高于正常数值。
- 24小时尿铜。 医务人员还可能给您测量 24 小时经尿液排出的铜量。威尔逊氏症患者的尿铜水平通常较高。被视为高数值的具体标准因实验室而异,但每天高于 40 至 100 微克(mcg)通常属于偏高。
- 其他肝脏检测。 可能进行其他检测,以检查肝脏功能状况。这类检测称为肝功能检测。但威尔逊氏症患者可能在肝功能和检测结果均正常的情况下依然出现肝受损。这被称为代偿性肝病。
眼科检查
在眼科检查中,眼科医生可以使用一种名为裂隙灯的特殊灯具来检查凯-弗环和向日葵样白内障。
凯-弗环呈金棕色或铜色,出现在虹膜(即眼睛的有色部分)的外边缘。这些环是由角膜中一处名为德塞梅膜的结构沉积过量铜而导致。角膜是覆盖瞳孔和虹膜的透明圆顶状薄膜。凯-弗环影响到大多数有神经系统症状的患者以及大约一半只有肝病症状的患者。
威尔逊氏症还会导致向日葵样白内障(一种特殊白内障)。这是由眼睛晶状体中的铜沉积引起的。
肝活检
在肝活检过程中,医务人员会将一根细针经皮肤穿刺插入您的肝脏,以采集一小份组织样本。接着在实验室中检测组织中的铜是否过量。铜含量高于 250 微克/克(mcg/g)肝脏干重是威尔逊氏症的体征。
基因检测
血液检测可以查找 ATP7B 基因突变,这种突变会导致威尔逊氏症。ATP7B 基因已知有数百种突变。其中最常见的突变之一是 p.H1069Q。如果您携带会导致威尔逊氏症的突变基因,则您的兄弟姐妹和子女也应该接受基因检测。早些发现该状况,就可以在出现症状之前开始治疗。
MRI
磁共振成像(MRI)是一项医学成像技术,使用磁场和计算机产生的射频波来生成人体器官和组织的详细图像。对于出现威尔逊氏症神经系统症状的患者,脑部 MRI 可能显示受铜沉积影响的脑区发生变化。约 10% 至 15% 威尔逊氏症患者的脑部 MRI 图像会呈现出“大熊猫脸征”。它表明威尔逊氏症已损害中脑(即脑的中部)。这一体征的名称源于 MRI 图像上呈现的深浅相间、类似熊猫脸的图案。
可能导致相似症状的状况
在诊断威尔逊氏症时,医务人员会考虑可能导致类似症状的其他状况。这有助于确保正确的诊断和治疗。
以下其他状况均由不同的基因变异所引起:
- 血色素沉着症。 像威尔逊氏症一样,血色素沉着症也可能累及肝脏。但两者的区别在于,威尔逊氏症涉及铜沉积,血色素沉着症涉及铁过量。
- 亨廷顿病。 威尔逊氏症和亨廷顿病都可能引起类似的运动和行为相关症状。但两者的区别在于,威尔逊氏症因铜沉积而累及肝脏和脑部,而亨廷顿病导致脑神经细胞随时间推移而退化,进而影响脑部。
- 无铜蓝蛋白血症。 无铜蓝蛋白血症和威尔逊氏症无关,尽管两者都影响与血液中的铜相结合的铜蓝蛋白。无铜蓝蛋白血症会导致肝脏出现铁沉积,而不是铜沉积。
- 门克斯病。 门克斯病也会影响身体对铜的利用。但威尔逊氏症不同于门克斯病。门克斯病会导致肝脏和脑部的铜水平偏低。威尔逊氏症会导致肝脏和脑部的铜水平偏高。
- 其他铜或铁代谢状况。 有些其他罕见遗传性状况可能影响铜和铁的平衡,但其遗传性病因各不相同。
导致所有上述状况的基因变异都与导致威尔逊氏症的基因变异不同。而且这些状况对人体产生的影响也不同。
治疗
为了治疗威尔逊氏症,医务人员可能首先推荐一种名为铜螯合剂的药物。这些药物会与铜结合,使器官把铜释放到血流中。然后肾脏把铜滤出并释放到尿液中。
后续治疗会侧重于预防铜再次沉积。通常采用含锌药物进行预防。肝损伤严重者可能需要接受肝移植。
威尔逊氏症是否能被治愈?
治疗可以防止威尔逊氏症进一步损害身体,且可以改善某些症状。药物不能治愈威尔逊氏症。肝移植不能治愈导致威尔逊氏症的基因变异。但是,由于供肝没有突变的基因,因此它或许可以在不进行更多治疗的情况下正确处理铜。如果威尔逊氏症能在早期发现并得到治疗,则患者能过上充实的生活并达到正常的预期寿命。
药物
如果使用药物治疗威尔逊氏症,除非进行肝移植,否则您需要终身使用。
用于清除铜的螯合剂
通常首先使用这些药物,作为快速降低铜水平的初步治疗:
- 青霉胺(Cuprimine、Depen)。 青霉胺有时也被称为 D-青霉胺,是一种将多余的铜从体内清除的药物。它可能引发严重的副作用,包括皮肤和肾脏问题。它还可能导致或加重神经系统症状,最常见于已经有神经系统症状的患者。还可能削弱骨髓充分生成红细胞和血小板的功能。如果您对青霉素过敏,应慎使用青霉胺。由于青霉胺会削弱维生素 B6(又称吡哆醇)的效用,因此您还需要使用小剂量的 B6 补充剂。
- 曲恩汀(Cuvrior、Syprine)。 这是另一种将多余铜从体内清除的药物。其作用类似青霉胺,但副作用通常更少。然而,使用曲恩汀仍有可能加重神经系统症状。
用于阻止铜吸收的锌疗法
醋酸锌(Galzin)可以阻止身体吸收食物中的铜。该药物通常用于维持治疗,以防止在青霉胺或曲恩汀初始治疗后再次出现铜沉积。如果您不能使用青霉胺或曲恩汀,或者您未表现出任何症状,则可能使用醋酸锌作为主要治疗药物。醋酸锌最常见的副作用是胃部不适。
医务人员还可能会推荐有关治疗威尔逊氏症其他症状的方法。
手术
活体肝移植
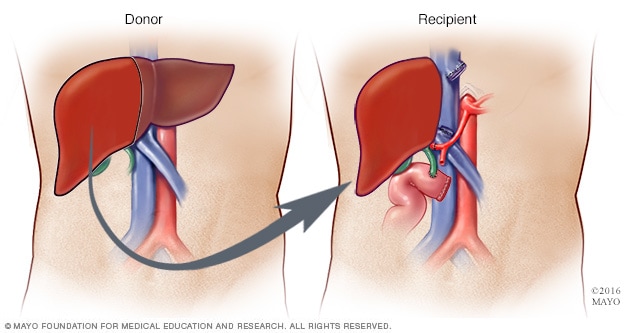
活体肝移植
在活体肝移植期间,外科医生会取下约 40%-70% 的供肝并将其植入受者体内。
如果肝脏受损严重而导致肝衰竭,或者肝脏损伤无法用药物逆转,则您可能需要接受肝移植。在肝移植手术期间,外科医生切除受损的肝脏,植入捐献者的健康肝脏。
大多数移植的肝脏来自于已故捐献者。有时,肝脏可能来自于活体捐献者,比如家庭成员。在此情况下,外科医生会切除受损的肝脏,并植入活体捐献者的部分肝脏。
生活方式与家庭疗法
管理威尔逊氏症需要终身用药,从而清除体内多余的铜并阻止过量铜沉积,还需要进行自我护理,以确保在饮食中不摄入过多的铜。
如果您被告知要限制饮食中的铜,则可能包括限制水、补充剂和食物中的铜。
水
如果您家中使用铜管,做饭用水或饮用前先放一会,等水变凉后再用。如果您使用井水,则对水质进行铜检测,或使用去除微量元素的过滤器。
补充剂
请务必避免使用含铜的复合维生素或补充剂。
食物
如果您患有威尔逊氏症,请咨询医护团队,了解如何调整饮食以满足任何必要的饮食限制并符合饮食指南。
医护团队很可能建议您限制铜的摄入量。但合适的摄入量可能取决于您所处的治疗阶段以及其他个人健康因素。例如,最初可能会要求您每天的铜摄入量不要超过 1 毫克(mg)。之后,可能请您在维持治疗阶段摄入一定量的铜,例如每天 2 mg 或更少。
含铜量高的食物
如果您患有威尔逊氏症,医生可能会建议您避免或限制食用以下食物:
- 肝脏和其他动物内脏。
- 贝类和虾。
- 羊肉。
- 鹅肉、鸭肉和鹌鹑肉。
- 豆腐、大豆蛋白和豆浆。
- 干豆。
- 蘑菇。
- 红薯和其他带皮土豆。
- 果干。
- 大豆粉、麸皮谷物和玉米粒。
- 坚果和果仁。
- 巧克力。
- 矿泉水。
含铜量低的食物
如果您患有威尔逊氏症,医护团队可能会告诉您,您可以多吃以下食物:
- 白肉(鸡肉和火鸡肉)。
- 鳕鱼、扇贝、大比目鱼、金枪鱼和鳟鱼。
- 蛋类、黄油和人造黄油。
- 奶酪、农家奶酪和酸奶油。
- 杏仁奶、牛奶和酸奶(非巧克力味)。
- 抱子甘蓝、西兰花和卷心菜。
- 菜花、菠菜和青椒。
- 洋葱。
- 香菇和金针菇。
- 苹果、蓝莓、樱桃、李子、甜瓜、草莓和西瓜。
- 咖啡和碳酸饮料。
有些健康食物含有适量的铜,可以少量食用。请向医护团队咨询哪些饮食指南适合您。
患有威尔逊氏症是否仍能正常生活?对此产生疑问或担忧实属正常。开始终身用药和培养新的饮食习惯,可能给您带来很大压力。请给自己一些时间做出调整,并告知医护团队您的担心。通过早期诊断、适当的医学治疗和自我护理,大多数威尔逊氏症患者可以过上健康的生活,知道这一点也可能会有所帮助。
准备您的预约
您可能需要先到初级卫生保健医务人员处就诊。之后,可能将您转诊给专门治疗肝病的医务人员(肝病专科医生)。
您能做些什么
约诊时,请询问您是否需要提前做准备,例如在血液检测前调整饮食。
列出以下内容可能会有所帮助:
- 您的症状以及症状开始的时间。
- 重要个人信息,包括重大压力、其他健康状况以及任何威尔逊氏症家族史。
- 您使用的所有药物、维生素或补充剂,包括剂量。
- 您要向医务人员咨询的问题。
尽量请他人陪同就诊,他们可以帮您记住医务人员提供的信息。
如果您认为自己可能患有或被告知患有威尔逊氏症,您可能要向医务人员咨询一些问题,比如:
- 我需要做哪些检查才能确诊威尔逊氏症?
- 您需要哪些家族史详细信息?
- 威尔逊氏症是如何长期治疗和监测的?
- 您推荐哪种治疗方法?
- 这种治疗有哪些副作用?
- 如何才能以最优方式同时管理威尔逊氏症和其他健康状况?
- 我需要限制食用的食物种类吗?
- 我应该去看专科医生吗?如果是,应该去看哪个专科?
- 我的兄弟姐妹或子女是否应该接受威尔逊氏症筛检?
- 我的家人应该去看哪个专科的医生?
- 有没有我可以带走的手册或其他印刷材料? 您推荐哪些网站?
如有任何其他疑问,请务必提出。此外,如果您的家族中有人患有威尔逊氏症或出现不明原因的肝脏、神经系统症状或心理健康问题,请务必告知医务人员,因为这种疾病具有家族聚集性。
医生可能做些什么
医务人员可能会问一些问题,例如:
- 您的症状是持续存在,还是时有时无?
- 您的症状有多严重?
- 这些症状持续多久了?
- 有没有什么因素似乎会令您的症状好转或加重?
- 您是否有其他家人患有威尔逊氏症?
Dec. 27, 2025