诊断
垂体瘤通常不易被察觉或检测出。分泌激素的肿瘤被称为功能性腺瘤。体积较大的肿瘤被称为大腺瘤。这两种肿瘤都可能引发与其他健康状况类似的症状。这些肿瘤也往往会随时间推移而缓慢生长。
不分泌激素的小垂体瘤(称为无功能微腺瘤)通常不会引起任何症状。这类小肿瘤通常是在因其他原因而进行的影像学检查(如 MRI 或 CT 扫描)中被发现。
垂体瘤与颅咽管瘤
垂体瘤和颅咽管瘤都长在垂体附近,可能引起头痛和视力变化等类似症状。它们也都可能影响激素水平。这些相似之处使人容易将其混淆,但二者并不相同。
垂体腺瘤始于垂体的激素分泌细胞。腺瘤可能产生过多的激素。许多垂体腺瘤采用内镜手术治疗。有些类型则使用药物治疗。
颅咽管瘤生长于垂体柄附近的胚胎残余组织。这类肿瘤往往含有囊肿。颅咽管瘤不会分泌激素,但可能改变正常的激素功能。颅咽管瘤的治疗通常包括手术和放疗。MRI 和 CT 扫描可用于帮助区分这两种状况。
为检查垂体瘤,医务人员可能会与您讨论您的个人及家族病史,并对您进行体格检查。用于检测垂体瘤的检查还可能包括:
-
血液检测。 血液检测可显示体内某些激素的水平是否过高或过低。在某些情况下,高激素水平可能足以让医务人员做出垂体瘤诊断。
对于皮质醇等其他激素,则可能需要进行更多检测,以确认高激素水平的原因是垂体瘤还是其他状况。
如果检测结果显示激素水平过低,则需要进行其他检查(通常是影像学检查),以确定这些检测结果是否由垂体腺瘤所致。
- 尿液检测。 尿液检测可以帮助检查一种会分泌过多 ACTH 的垂体腺瘤。ACTH 过多会使体内皮质醇水平升高,从而导致库欣病。
- 脑部 MRI 扫描。 磁共振成像扫描(MRI 扫描)可以生成身体器官和组织的详细图像。脑部 MRI 可以帮助检测垂体瘤,并显示其位置和大小。在 MRI 检查期间,会将少量造影剂注入静脉。造影剂随血液流动,有助于更清晰地显示某些组织。
- 脑部 CT 扫描。 计算机体层成像扫描(CT 扫描)使用一系列 X 线来生成横截面图像。CT 扫描在垂体瘤检查中的使用频率不如 MRI 扫描。然而,在制定手术计划时,CT 扫描可能会有所帮助。
- 视力检查。 有些垂体瘤可能会影响视力,尤其是侧面视力。眼科检查可以帮助检查视力是否受到影响。
垂体瘤在 MRI 图像上是什么样子?
体积较小的肿瘤被称为微腺瘤,在垂体 MRI 中通常显示为一个微小点部。肿瘤对造影剂的吸收速度和垂体其他部分有所不同。因此,在刚注射造影剂之后,这个小肿瘤点在图像上通常显得更暗。体积较大的肿瘤被称为大腺瘤,可能使垂体看起来更大,并且可能把垂体其他部分挤向一边。它还可能压迫周围组织,例如帮助您视物的神经。
如何通过 MRI 识别垂体瘤?
MRI 扫描使用薄层生成极详细的脑部图像。医务人员在注射造影剂之前和之后拍摄图像,以帮助识别肿瘤。如果肿瘤体积很小,可以在注射造影剂之后立即通过一种快速扫描非常迅速地生成多张图像。微腺瘤吸收造影剂的速度较慢,因此在刚注射造影剂之后,它们看起来比垂体的其他部分更暗。
体积较大的肿瘤通常容易被发现。MRI 可显示肿瘤与视神经和邻近血管之间的距离。通过 MRI 确定肿瘤部位,对于手术规划以及在治疗期间保护视力和整体健康而言至关重要。
针对垂体腺瘤的血液检测:检查哪些项目?
血液、尿液和唾液检测可检查以下两项:
- 肿瘤产生过多激素。 常规检测项目包括测定催乳素、介导生长激素发挥作用的胰岛素样生长因子-1(IGF-1)和甲状腺功能(TSH 和游离 T4)。皮质醇和 ACTH 检测可评估垂体和肾上腺分泌和调控皮质醇的功能。皮质醇是一种与应激和新陈代谢有关的激素。
- 垂体激素水平偏低。 血液检测可测定皮质醇、游离 T4 和 TSH、性激素(例如睾酮或雌二醇)以及黄体生成素(LH)和卵泡刺激素水平,还可以检测 IGF-1 水平,以查找可能需要治疗的激素缺乏症。
医务人员可能将您转诊给激素紊乱专科医生(内分泌科医生),以进行更多检查。
治疗
大多数垂体瘤不是癌症,如果不引起症状,可能不需要治疗。在许多情况下,定期监测就足够了。
如果需要治疗,医护团队会考虑多项因素,包括肿瘤的类型、大小和位置、生长速度,以及肿瘤是否影响激素水平。您的年龄和整体健康状况也有助于指导治疗决策。
治疗目标在于:
- 使激素水平恢复到正常范围。
- 避免对垂体造成更多损害,使其恢复正常功能。
- 缓解由肿瘤压迫引起的症状或防止其恶化。
如果垂体腺瘤需要治疗,医护团队可能会建议采用手术、药物治疗或放射疗法。您将获得专家团队的支持,该团队可能包括:
- 激素紊乱专科医生(内分泌科医生)。
- 脑外科医生(神经外科医生)。
- 鼻和鼻窦外科医生(ENT 外科医生)。
- 放疗专科医生(放射肿瘤科医生)。
垂体瘤会自行缩小吗?
这并不常见。在极少数情况下,观察到被称为微催乳素瘤的肿瘤自行缩小甚至消失。更多情况下,分泌催乳素的肿瘤通过药物治疗而缩小。
手术
垂体瘤可以通过手术切除进行治疗。这种手术有时也被称为肿瘤切除术。
多大的垂体瘤应该切除?
没有规定多大的肿瘤需要切除。如果肿瘤出现以下情况,通常建议进行手术:
- 压迫视神经或影响视力。
- 导致体内某些激素分泌过多。
- 挤压垂体,降低激素水平。
- 治疗后继续生长。
- 出血并引起症状。
- 引起其他症状,如头痛或面部疼痛。
肿瘤体积越大,越有可能压迫周围组织。为了确定手术是否为最佳治疗方法,医护团队会考虑多种因素。这些因素包括症状、激素检测、生长情况和扫描结果,而不仅仅考虑肿瘤大小。
术后结果通常取决于腺瘤的类型、大小和位置,以及肿瘤是否已生长到侵入周围组织。
切除垂体瘤的手术包括经鼻蝶手术和开颅术。
经鼻蝶手术
内镜经鼻蝶手术
内镜经鼻蝶手术
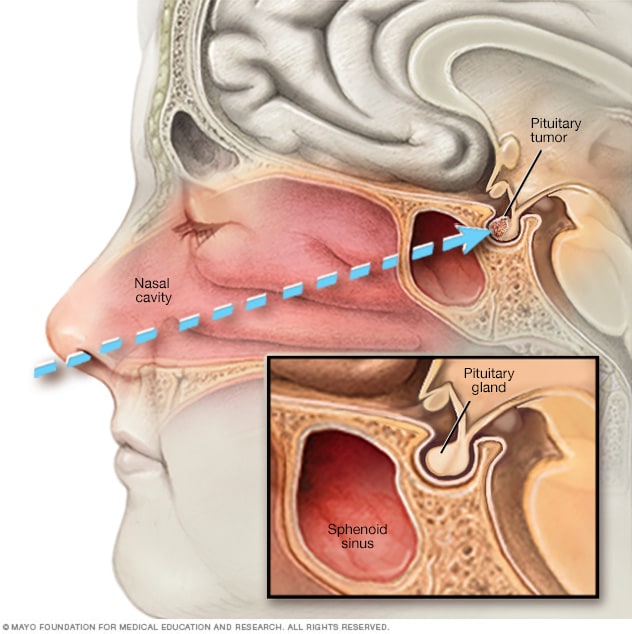
进行内镜经鼻蝶手术时,医生把一种手术器具经鼻孔放入鼻腔,沿着鼻中隔探入,接近垂体瘤。
经鼻蝶手术是用于治疗垂体瘤的最常见医疗程序。外科医生可以通过这项手术经鼻腔触及肿瘤。
在手术过程中,外科医生经鼻孔切除肿瘤。手术不需要任何外部切口,也不会留下可见的瘢痕。这项手术过程中,不会触碰到脑部组织。脑外科医生通常会与鼻和鼻窦科专家合作,安全地进行此项手术。
体积较大的垂体瘤可能较难通过该手术切除,尤其是在肿瘤已经扩散至周围神经、血管或其他脑区的情况下。
垂体腺瘤经蝶窦切除术是否与内镜经鼻蝶手术相同?
总体而言,是的。经蝶窦切除术意味着外科医生经由鼻腔和蝶窦触及垂体。这条手术入路可通过显微镜或内镜完成。内镜经鼻蝶手术以同样入路触及垂体,但使用一个柔性小摄像头。这种方案提供了广角近距离视野。
经颅手术
经颅手术有时被称为开颅术。在垂体瘤的治疗中,这种手术的使用频率低于经鼻蝶手术。
对于体积较大的垂体瘤,可能建议进行经颅手术。如果肿瘤已经扩散到周围神经或脑组织,也可能建议进行这项手术。该手术使外科医生能够更好地看到整个肿瘤及其周围的脑组织。在经颅手术过程中,外科医生会在头皮上做一个切口,经由颅骨上部切除肿瘤。
经鼻蝶手术和经颅手术一般都比较安全。并发症并不常见。但和所有手术一样,也存在风险。垂体瘤手术后的并发症可能包括:
- 出血。
- 感染。
- 麻醉药物(使您在术中进入类似睡眠状态的药物)的副作用。
- 短暂性头痛和鼻塞。
- 脑损伤。
- 视力变化,例如复视或视力丧失。
- 垂体受损。
- 一种被称为尿崩症的状况。
尿崩症出现在垂体无法分泌足够的血管升压素(一种激素)时。这种激素有助于保持体内液体平衡。如果血管升压素水平过低,您的身体会产生过多的尿液,这可能会导致极度口渴和脱水。垂体瘤切除术后出现的尿崩症一般为暂时性的,通常不经治疗也可在几天内自行消退。如果该状况持续时间更长,医护团队可能会建议使用药物来替代缺失的激素。在大多数情况下,该状况会在几周或几个月后消退。
如果医务人员建议采用手术治疗垂体瘤,请提出问题以帮助您做好准备。了解哪一种手术可能最适合您。咨询可能出现的风险和副作用。另请询问恢复期间的预期情况。
垂体瘤手术的生存率是多少?
预后和成功率取决于肿瘤的类型、大小、扩散部位以及手术团队的经验。对于许多患有激素分泌型小肿瘤的患者,激素水平在手术后会恢复正常。大约 70% 到 90% 的库欣病患者在经验丰富的手术中心接受手术后会得到缓解。
手术切除压迫视神经的肿瘤后,视力通常会得到改善。约 70% 至 90% 有视力问题的患者的视力有所改善。但是,如果视神经长时间受压,则完全恢复的可能性较小。有些肿瘤,特别是体积较大或具有侵袭性的肿瘤,在手术后需要进行药物或聚焦放射治疗。有时,需要联合使用药物和放射治疗。
放射疗法
放射疗法使用高能放射源治疗垂体瘤。该疗法可能在手术后使用,如果不选择手术,则可能单独使用。
如果垂体瘤出现以下情况,放射疗法可能会有所帮助:
- 手术无法完全切除。
- 术后复发。
- 导致药物无法缓解的症状。
垂体腺瘤放射疗法的目标是控制腺瘤生长或阻止腺瘤分泌激素。
可用于治疗垂体瘤的放射疗法包括:
- 立体定向放射外科治疗。 这种放射疗法通过单剂量辐射聚焦来治疗肿瘤。虽然这是一项外科手术,但无需做切口。为了指导治疗,医务人员使用脑成像技术并在您的头部放置一个特制框架。框架帮助辐射束精确瞄准肿瘤,会在手术后立即移除。由于能够使辐射非常精确地对准肿瘤,因此周围健康脑组织受到的辐射极少。这种方法可降低损伤健康组织的风险。
- 外照射疗法。 这种方法也被称为分割放射治疗。该疗法在一段时间内分多次给予小剂量辐射,而不是一次照射就给予全部剂量。通常每周照射五次,持续 5 到 6 周。
- 调强放射治疗(IMRT)。 这种放射疗法使用计算机从多个角度调节肿瘤周围辐射束的形状和方向。可以控制辐射束的强度,以减少对周围健康组织的损伤。
- 质子束疗法。 这种放射疗法使用被称为质子的带正电离子来靶向肿瘤。质子束在肿瘤内释放能量后停止运动。这有助于保护周围健康组织,并可能降低出现副作用的风险。质子束疗法需要使用特殊设备,且尚未广泛应用。
垂体腺瘤放射疗法的潜在副作用和并发症可能包括:
- 垂体损伤,这可能会限制身体分泌激素的功能。
- 垂体周围的健康组织损伤。
- 视神经受损引起的视力变化。
- 垂体周围的其他神经损伤。
- 患脑肿瘤的风险略有增加。
如果医护团队建议采用放射疗法,放射肿瘤科医生可以帮助您了解可能的益处和风险。垂体腺瘤放射疗法起效缓慢,因此可能需要数月或数年才能看到整体疗效。副作用也可能需要很长时间才会出现。正因如此,治疗后定期检查以观察是否有任何激素变化或其他问题至关重要。
药物
某些垂体瘤可能使用药物治疗。药物可以帮助降低肿瘤分泌的激素量。在某些情况下,药物还可能有助于缩小肿瘤。
用于治疗分泌催乳素的垂体瘤的药物
用于治疗分泌催乳素的肿瘤的药物通常可以达到所有治疗目标。这些目标包括使激素水平恢复到正常范围、防止垂体进一步受损,以及缓解肿瘤压迫导致的症状。采用药物治疗后,许多患者可能无需接受手术或放射治疗。药物通常还可能使肿瘤缩小。以下药物用于减少垂体腺瘤分泌的催乳素。
可能的副作用包括:
- 头晕。
- 困倦。
- 胃部不适或呕吐。
- 心境障碍,包括抑郁。
- 头痛。
- 无力。
在使用这些药物期间,部分患者还可能出现难以自控的行为,例如赌博。这类行为被称为冲动控制障碍。使用这些药物的育龄患者应向医务人员咨询避孕方案。还应告知医务人员自己是否正考虑怀孕。
药物治疗分泌促肾上腺皮质激素的垂体瘤
分泌促肾上腺皮质激素(ACTH)的肿瘤会使身体产生过多皮质醇。这可能导致一种被称为库欣病的状况。可能降低皮质醇水平的药物包括:
- 酮康唑。
- 美替拉酮(Metopirone)。
- 奥唑司他(Isturisa)。
这些药物可能产生的一些副作用包括胃部不适、头痛和疲劳。
对于同时还患有 2 型糖尿病或血糖控制不佳的患者,另一种名为米非司酮(Korlym、Mifeprex)的药物可用于治疗库欣病。米非司酮的作用并不是减少身体产生的皮质醇,而是阻止皮质醇对身体组织产生影响。
米非司酮的副作用包括:
帕瑞肽(Signifor)有助于减少垂体腺瘤分泌的 ACTH,从而降低皮质醇水平。每天注射两次。如果手术切除腺瘤无效或不适用,医务人员可能会建议使用帕瑞肽。
帕瑞肽可能产生的副作用包括:
- 腹泻。
- 胃部不适。
- 高血糖。
- 头痛。
- 胃疼。
- 胆结石。
生长激素型垂体瘤
有两类药物可以治疗分泌生长激素的垂体瘤。如果手术不能使生长激素水平恢复到正常范围,医务人员通常会开以下这些药物。
垂体激素替代治疗
垂体有助于控制许多重要的身体功能,如生长和生殖。垂体肿瘤或其切除方法有时可能会导致垂体功能发生变化。如果导致激素水平降得太低,则您可能需要接受激素替代治疗,以帮助您将激素水平恢复到正常范围。
激素替代治疗可能需要持续一小段时间,也可能终身需要。有时在治疗结束很久之后才需要激素替代治疗。这强调了治疗后长期进行定期复诊的必要性。
等待观察
在观察等待期(也称为观察期或延迟疗法),您可能需要接受定期复诊检查,以观察肿瘤是否生长或激素水平是否发生变化。如果腺瘤没有引起任何症状或健康问题,这可能是一个不错的选择。请向医务人员咨询观察等待和治疗对您的病情分别有哪些益处和风险。
临床试验
探索 Mayo Clinic 的研究 测试新的治疗、干预与检查方法,旨在预防、检测、治疗或控制这种疾病。
生活方式与家庭疗法
患有垂体腺瘤可能会带来很多困难。但您可以采取以下措施,以维持自己的最佳状态,并改善整体健康:
- 定期进行身体活动。 对于垂体腺瘤患者来说,运动可以提升精力水平,并改善睡眠和情绪。请询问医护团队哪类活动对您来说是安全的,特别是当您正处于手术或放疗的恢复期。
- 健康饮食。 均衡的饮食可在治疗和恢复期间为您的身体提供支持。如果您患有会导致库欣病的垂体腺瘤,请咨询医护团队,了解保护骨骼健康的方法。您可能需要摄入更多的钙和维生素 D 来帮助保持强健的骨骼。
- 遵循治疗计划。 确保完全按照处方用药。参加所有复诊,以便医护团队可以跟踪您的病程进展,并在需要时调整治疗方案。
- 观察激素引发的症状。 垂体腺瘤可能会影响激素水平。如果您注意到体重、情绪、精力水平、视力或月经周期发生变化,请告知医务人员。
妥善处理与支持
得到患有垂体瘤的诊断时,产生疑问是正常反应。这个过程可能让人感到不堪重负,甚至感到恐惧。详细了解您所患的状况可以帮助您增强信心和掌控感。
您可能会发现,与有类似病情的人分享您的感受会有所帮助。查看您所在地区是否有垂体瘤患者互助组。医院经常支持组织这些互助团体。请咨询医务人员,了解您所在地区是否有团体或其他资源可以提供您所需的支持。
接受垂体瘤手术后,患者的生活会是怎样的?
大多数人几天内即可出院。术后常见短暂的鼻塞、轻微头痛和喉咙痛。您需要定期随访,检查伤口愈合情况、视力状况和激素水平。部分患者需要接受短期或长期激素替代治疗,并且将通过 MRI 复查监测肿瘤部位。
垂体瘤手术后需要多长时间才能恢复?
恢复情况因人而异。在术后几周内,许多患者可以恢复日常活动,尽管鼻和鼻窦仍在愈合中。关于这一期间如何提举物品、擤鼻涕和运动。医护团队将提供具体指导。
有些患者在垂体瘤手术后出现体重下降吗?
具体取决于肿瘤类型。在成功治疗库欣病后,随着皮质醇水平恢复至正常水平,体重通常会随着时间的推移而下降。如果患有其他类型的肿瘤,体重可能变化不大。如果出现任何体重快速变化,请告知医护团队,以检查激素水平和药物。
是否有患者在垂体瘤手术后出现性格变化?
在手术后,激素水平和您的身体都在恢复中,因此,情绪变化可能会持续一段时间。随着激素达到正常水平,大多数患者会在术后几周到几个月内有所改善。接受库欣病治疗的患者,可能在高皮质醇水平恢复期间出现疲劳、情绪低落或易激惹。或许需要长达一年的时间才能让您感觉恢复到以前的状态。请告知医护团队您的情绪或思维问题是否严重或持续存在。治疗和咨询可能会有帮助。
垂体瘤患者需要避免食用哪些食物?
目前没有针对垂体瘤的特殊饮食。均衡饮食适合大多数患者。一些用于治疗垂体瘤的药物会与食物或其他药物产生相互作用,因此请遵循医务人员给出的具体指导。
垂体瘤切除后的预期生存期多长? 如果肿瘤癌变,预期生存期会改变吗?
大型研究表明,在垂体腺瘤(一种良性肿瘤)确诊者中,超过 80% 的患者存活超过 10 年。研究确实表明,如果通过手术完全切除肿瘤,激素水平恢复正常,并且患者年轻且没有其他健康问题,则大多可以达到正常寿命。这一生存率与治疗无关。
然而,并没有一个可靠数字能说明患者在单独接受手术治疗后的生存期,因为研究并非总是针对仅接受手术治疗的患者而开展。
垂体癌(垂体腺癌)非常罕见。预后因人而异,但生存期明显低于垂体腺瘤。研究表明,癌症扩散后的中位生存期在 1.5 至 3.6 年之间。
准备您的预约
您可能需要先到初级卫生保健医务人员处就诊。您可能会被转诊给一位或多位专科医生。这些专科医生可能包括眼病治疗医生(眼科医生)、脑外科医生(神经外科医生)或激素专科医生(内分泌科医生)。
以下信息可以帮助您做好就诊准备。
您能做些什么
约诊时,请询问是否需要提前做准备,例如在某项检查前禁食。请列出以下内容:
- 您的症状,包括可能看似与约诊原因无关的任何症状。
- 关键个人详细信息,包括重大压力、近期的生活变化和家族病史。
- 您使用的所有药物、维生素或补充剂,包括剂量。
- 要向医务人员咨询的问题。
如果可能,请家人或朋友陪同就诊。陪同者可以帮助您记住您在就诊期间获得的信息。
对于垂体瘤,需要向医务人员咨询的问题包括:
- 我的症状或状况可能是什么原因引起的?
- 是否还有其他可能的原因?
- 我应该看哪个科室的专科医生?
- 我需要做哪些检查?
- 您推荐哪些治疗方法?
- 除了您的建议外,还有其他治疗选项吗?
- 我还有其他健康状况。我如何才能同时管理好这些状况?
- 有没有需要遵守的限制规定?
- 有没有我可以带走的手册或其他印刷材料? 您推荐哪些网站?
如果您想到任何其他问题,也可以提出。
医生可能做些什么
医务人员可能会问您一些问题。其中可能包括:
- 您何时开始出现症状?
- 您的症状是时有时无,还是一直存在?
- 您的症状有多严重?
- 您是否注意到有任何因素会改善您的症状?
- 您是否注意到有任何因素会加重您的症状?
- 您既往是否因为任何原因做过头部影像学检查?
- 您未来有怎样的生育计划?