March 12, 2022
Negative dysphotopsia (ND), an unwanted shadow in the temporal field after cataract surgery, occurs in approximately 12% of patients at one month after surgery, decreasing to 3% at one year. ND is a major source of patient dissatisfaction.
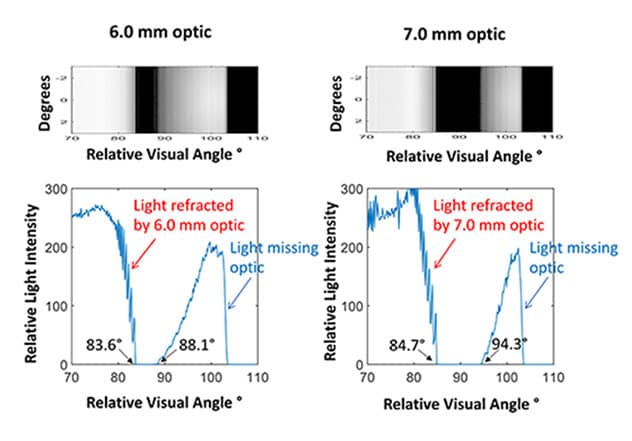
Profile of nasal retina using 6.0 and 7.0 mm optics
Profile of nasal retina using 6.0 and 7.0 mm optics
Simulated illumination profile of the nasal retina (70 to 110 degrees) using a 6.0 mm optic (left) and 7.0 mm optic (right). The shadow-like region is broader and shifted anteriorly onto more peripheral retina, or possibly off retina when using a 7.0 mm optic. Based on the Journal of Cataract & Refractive Surgery.
The intraocular lens (IOL) is thinner and smaller in diameter than the natural crystalline lens, and when placed in the capsular bag, a space is created between the posterior iris and the IOL that is not present in the phakic eye. These characteristics provide an opportunity for peripheral light rays to miss the IOL and nonphysiologically illuminate the peripheral retina. Additionally, a narrow shadow-like region may form in the nasal retina, bounded anteriorly by light missing the IOL and posteriorly by light refracted by the IOL. This shadow in the nasal retina is hypothesized to correspond to the bothersome temporal shadow seen in ND.
"It is thought that the perception of the ND shadow may be mitigated if the dark region of nasal retina is illuminated by redirected light, or if light missing the IOL is shifted anteriorly off the retina, or both," notes Michael A. Mahr, M.D., Ophthalmology, at Mayo Clinic in Rochester, Minnesota.
A recent clinical study by M. K. Bonsemeyer and others, published in the Journal of Cataract & Refractive Surgery in 2022, showed that enlarging an IOL hydrophobic optic from 6.0 mm to 7.0 mm significantly reduced ND symptoms at one month after cataract surgery. Based on those findings, Dr. Mahr and fellow researchers conducted a laboratory study using ray-tracing analysis to compare the influence of 6.0 mm and 7.0 mm IOL optic diameters on illumination of the peripheral retina. Their study was published in the Journal of Cataract & Refractive Surgery in 2022.
The researchers used Zemax OpticStudio software to generate simulated retina illumination profiles of the peripheral retina for an average pseudophakic eye with an in-the-bag biconvex IOL and a 2.5 mm pupil. Researchers compared ray-tracing diagrams and simulated retina illumination profiles using 6.0 mm and 7.0 mm optic-diameter IOL. Retinal locations were scaled to relative visual angles from 70 to 110 degrees horizontally.
Results
A low-refractive-index 7.0 mm optic increased the focused image field by 3 degrees when compared with a 6.0 mm optic. The width of the shadow also increased from 7 degrees to 10 degrees, which moved the outer edge of the shadow more peripherally by over 5 degrees.
"Consequently, the distinct narrow shadow seen with a 6.0 mm optic is enlarged and shifted peripherally with a larger 7.0 mm optic," says Dr. Mahr.
Calculations for a high-refractive-index optic showed similar changes. The shadow width increased from 5 degrees to 10 degrees, with the outer edge of the shadow moving peripherally 6 degrees.
"Our simulated illumination profiles confirm that light focused by the IOL, as well as nonphysiologic light that bypasses the IOL, is shifted peripherally when using a 7.0 mm optic compared with a 6.0 mm optic," says Dr. Mahr. "As a result, the narrow shadow seen with a 6.0 mm optic is broadened, and its anterior border is shifted onto more peripheral retina, or possibly off retina. This illumination change may be less bothersome or may allow easier neuroadaptation — thus explaining why ND rates are lower when using a 7.0 mm-diameter optic."
For more information
Bonsemeyer MK, et al. Dysphotopsia and functional quality of vision after implantation of an intraocular lens with 7.0 mm optic and plate haptic design. Journal of Cataract & Refractive Surgery. 2022;48:75.
Erie JC, et al. Effect of a 7.0 mm intraocular lens optic on peripheral retinal illumination with implications for negative dysphotopsia. Journal of Cataract & Refractive Surgery. 2022;48:95.
Refer a patient to Mayo Clinic.