Aug. 30, 2019
Mayo Clinic's cerebral spinal fluid (CSF) dynamics clinic provides a multidisciplinary, specialized approach to the management of idiopathic intracranial hypertension (IIH). Within a few days, patients can see a neurologist and neuro-ophthalmologist, have diagnostic testing, and see a neurosurgeon if needed. Timely diagnosis and treatment are essential for the optimal treatment of IIH.
"We have multiple specialists working side by side and early on to coordinate this care," says Jeremy K. Cutsforth-Gregory, M.D., a neurologist at Mayo Clinic in Rochester, Minnesota, who leads the CSF dynamics clinic. That group also provides a team approach to care for normal-pressure hydrocephalus and spontaneous CSF leaks.
IIH is often misdiagnosed, and standard surgical treatment with a shunt frequently requires one or more re-operations. Mayo Clinic has experience with sophisticated imaging and lumbar puncture to confirm the diagnosis, as well as venous sinus stenting for treatment. Most people with IIH are women between the ages of 15 and 50.
"Up to 40% of patients with this condition can have permanent vision loss," says John J. Chen, M.D., Ph.D., a neuro-ophthalmologist at Mayo Clinic's campus in Minnesota. "With early and accurate treatment, we can preserve their vision. That's why it is so important for them to be seen and treated in a timely manner."
Accurate diagnosis and stepwise treatment
At Mayo's CSF dynamics clinic, neurologists and neuro-ophthalmologists work together to confirm the diagnosis of IIH. The results of MRI, magnetic resonance venography (MRV) and lumbar puncture are carefully evaluated to exclude a diagnosis of tumor, venous sinus thrombosis, infection or inflammation.
"We find that as many as 40% of patients referred to us for IIH may not actually have the condition," Dr. Chen says. "A lot of patients are given a diagnosis of IIH based on having headaches and a single, spurious lumbar puncture that shows elevated pressure. However, the lumbar puncture might have been done in the wrong position or while the patient was not appropriately relaxed. Also, what has previously been considered an elevated opening pressure can be seen in normal patients."
Grade 4 papilledema
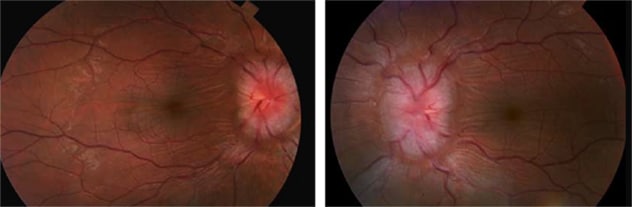
Grade 4 papilledema
Images show a grade 4 papilledema in a 27-year-old woman with idiopathic intracranial hypertension.
Once the diagnosis of IIH is confirmed, initial treatment focuses on lowering intracranial pressure to relieve papilledema. Depending on the degree of papilledema, medications such as acetazolamide might be tried. If the IIH is fulminant or medication fails to adequately reduce pressure, surgery is recommended.
The classic surgical treatment involves the implantation of a shunt. Although shunts can relieve pressure and papilledema, and sometimes headaches, they often clog or malfunction. "We can almost guarantee that patients will have a shunt failure within a handful of years — which means repeat surgeries or, at the very least, multiple scans and testing to prove that the shunt is still working," Dr. Cutsforth-Gregory says.
MRV shows transverse venous sinus stenosis (arrows)
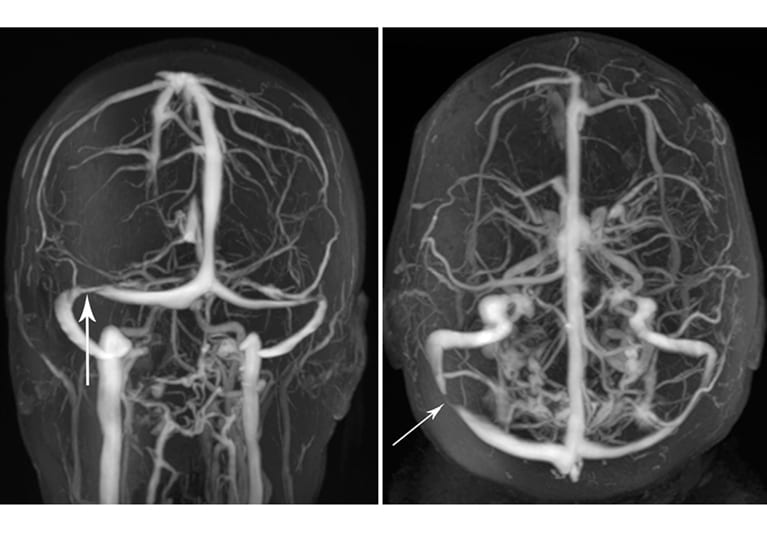
MRV shows transverse venous sinus stenosis (arrows)
Magnetic resonance venography (MRV) images show transverse venous sinus stenosis (arrows) in a 30-year-old woman with obesity and idiopathic intracranial hypertension. She subsequently underwent uncomplicated angioplasty and stenting of the right transverse sinus, which normalized a pressure gradient across the transverse-sigmoid sinus junction.
To avoid that scenario, Mayo Clinic often uses venous sinus stenting as a surgical option. The procedure involves inserting a catheter into the venous sinus and measuring the pressure above and below the transverse sinus stenosis that's typically associated with IIH. If a significant pressure gradient is detected, a stent is placed. "The gradient disappears, and intracranial pressure is normalized in a nontraumatic way. The papilledema almost always improves or resolves," says Giuseppe Lanzino, M.D., a neurosurgeon at Mayo Clinic's campus in Minnesota.
Managing headaches and obesity
Two-thirds of patients continue to have headaches after intracranial pressure is normalized and papilledema is resolved. The CSF dynamics clinic uses its multidisciplinary approach to manage the next phase of those patients' care.
"Headache is often the major complaint of patients with IIH. Once we've addressed the risk of vision loss, we want to help patients with their headaches," Dr. Cutsforth-Gregory says. About two-thirds of these headaches are migraines. "We use the standard migraine approaches, up to and including Botox. Ultimately, most of our patients have fewer headaches and improved quality of life," Dr. Cutsforth-Gregory says.
Because about 90% of people with IIH are obese, dietitians and nutritionists are often involved. "The initial intervention to protect patients' vision is really a bridge to their losing weight to prevent IIH from recurring," Dr. Cutsforth-Gregory says. In addition, Mayo Clinic endocrinologists help manage care for patients with polycystic ovary syndrome, which can occur with obesity and IIH.
To learn more about the optimal treatment of IIH, Mayo Clinic is participating in the Surgical Idiopathic Intracranial Hypertension Treatment Trial (SIGHT), a randomized, multicenter clinical trial comparing treatments for IIH involving moderate to severe vision loss. Study participants will receive medical therapy, medical therapy plus optic nerve sheath fenestration or medical therapy plus cerebral spinal fluid shunting.
Other research efforts include a clinical trial investigating the use of MR elastography (MRE) to evaluate raised intracranial pressure. "We think raised pressure will cause the brain to become stiffer. MRE might provide a noninvasive alternative to lumbar puncture for detecting raised intracranial pressure," Dr. Chen says.
An additional project, in conjunction with NASA, is investigating why astronauts — who aren't obese — often develop papilledema in outer space. "We're looking at astronauts and more-typical patients with IIH to see if there's a genetic polymorphism that they might share that predisposes them to papilledema. Not all people who are obese get papilledema, and we'd like to find a clear cause," Dr. Chen says. "The field is evolving — it's pretty exciting. Having a plethora of research collaborators helps us advance the field, while our clinical approach through the CSF dynamics clinic helps us to provide optimal care for patients."