Sept. 12, 2018
Mayo Clinic has enhanced its capability to offer minimally invasive surgery for craniosynostosis, even for babies with multiple sutures or syndromic conditions. "The long-term results we're seeing from minimally invasive surgery are as good if not better than from open surgery," says Edward S. Ahn, M.D., a pediatric neurosurgeon at Mayo Clinic in Rochester, Minnesota. "We're able to achieve the same results but with smaller incisions and shorter hospital stays for infants.
"The less invasive procedure can be performed early," he adds. "With traditional open surgery, we've typically waited until at least 6 months of age before performing the procedure so that the baby will be larger and better able to tolerate major surgery. But the earlier surgery is performed, the better the results in general."
For optimal results, minimally invasive surgery for craniosynostosis should be performed before age 3 months. "However, there are circumstances — such as if the abnormality is milder — that allow us to do minimally invasive surgery successfully even for slightly older children," Dr. Ahn says.
Open craniosynostosis surgery takes several hours. "Afterward, we monitor the babies, usually in the ICU, for at least one night and then in the hospital for several more days because of the invasiveness of the procedure and the risk of blood loss," Dr. Ahn says. "With the less invasive procedure, we've been happy to have the babies monitored just overnight in a regular unit and go home the next day."
Single surgery for children with syndromic conditions
Mayo Clinic treats about 400 babies with craniosynostosis or other craniofacial disorders each year. Minimally invasive surgery can be effective even for children with syndromic craniosynostosis. Typically, those patients — who account for 8 to 24 percent of all children with craniosynostosis — have had open surgery. Among the limited number of patients who have had an endoscopic procedure, many have needed subsequent calvarial remodeling.
But in a study published in the July 2017 issue of Journal of Neurosurgery: Pediatrics, Dr. Ahn and colleagues found that early endoscopic suturectomy followed by helmet therapy is sufficient to treat about half the children with syndromic craniosynostosis.
"Although the chance of needing repeat surgery is higher in children with syndromic craniosynostosis than in babies with the nonsyndromic condition, some can be treated with just that single endoscopic procedure," Dr. Ahn says. "Even if subsequent open surgery is needed, the early endoscopic procedure might allow time for the brain and skull to grow and develop, delaying the need for open remodeling until the child is older and can better tolerate the procedure."
To minimize blood loss during endoscopic craniosynostosis surgery, Dr. Ahn uses an ultrasonic device to remove bone. "That instrument minimizes bleeding from the bone," he notes.
Single incision endoscope-assisted sagittal strip craniectomy
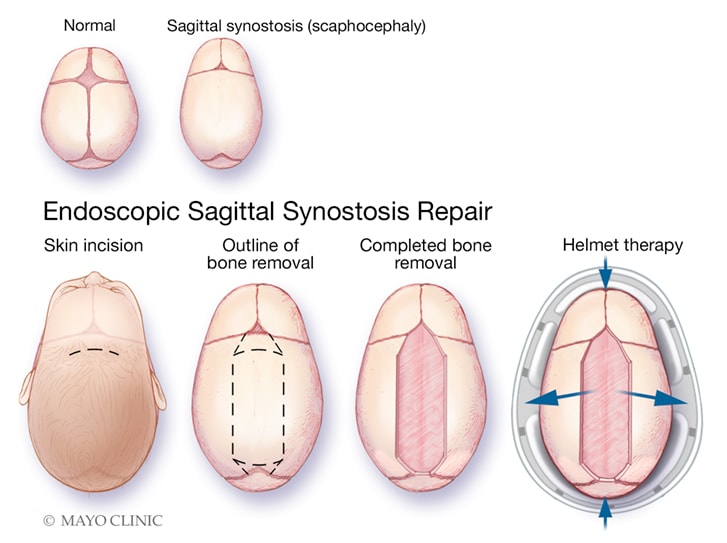
Single incision endoscope-assisted sagittal strip craniectomy
Illustration depicts the surgical technique for single incision endoscope-assisted sagittal strip craniectomy. The upper panel shows the elongated skull shape that results from sagittal synostosis. The lower panel shows the removal of the abnormal bone through a single incision followed by correction of the head shape with the aid of a molding helmet.
For babies with sagittal synostosis, Dr. Ahn has experience performing endoscopic suturectomy with a single incision. As described in the January 2017 issue of Child's Nervous System, the novel technique decreases blood loss associated with the traditional two-incision procedure while allowing for excellent clinical outcomes. The average operative time for the procedures among cases studied was 87 minutes.
"Endoscopic incisions are small. But perfecting our technique to eliminate one of those incisions has made the endoscopic procedure even less invasive," Dr. Ahn says.
Helmet therapy after endoscopic surgery has historically lasted as long as a year to 18 months. "We're studying the optimal time for helmet use, to try to minimize it if possible," Dr. Ahn says. "The need for helmet use is probably not as long as we've generally done. I would estimate that the ideal time for most of our patients is six to eight months. For all of our patients with craniosynostosis, we're trying to be smarter and less invasive."
Learn more about Dr. Ahn and Mayo Clinic's approach to pediatric neurosurgery by viewing Minimally invasive surgery for craniosynostosis requires early diagnosis and intervention.
For more information
Hersh DS, et al. Endoscopic surgery for patients with syndromic craniosynostosis and the requirement for additional open surgery. Journal of Neurosurgery: Pediatrics. 2017;20:91.
Iyer RR, et al. Single incision endoscope-assisted surgery for sagittal craniosynostosis. Child's Nervous System. 2017;33:1.