April 24, 2014
Palpation of the thyroid gland
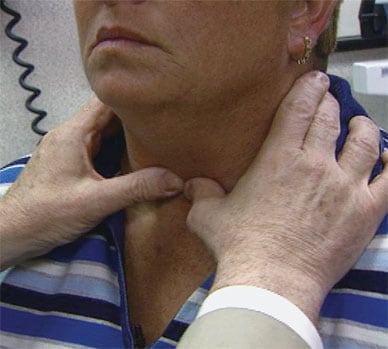
Palpation of the thyroid gland
Palpable nodules are found in 4 to 7 percent of the adult U.S. population.
Ultrasound-guided fine-needle aspiration of a thyroid nodule

Ultrasound-guided fine-needle aspiration of a thyroid nodule
Guidelines from the American Thyroid Association specify that the evaluation of a thyroid nodule should include fine-needle aspiration of nodules that meet the appropriate size and ultrasound criteria.
Thyroid cytology of a specimen of papillary thyroid carcinoma
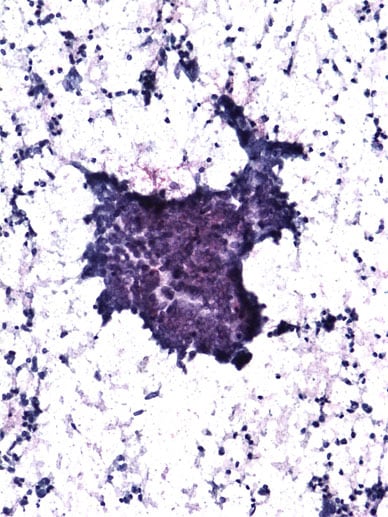
Thyroid cytology of a specimen of papillary thyroid carcinoma
Thyroid cytology of a specimen of papillary thyroid carcinoma showing papillary architecture and nuclear enlargement with crowding of classic papillary thyroid cancer (Papanicolaou stain, original magnification times 100)
Thyroid nodules are common, with palpable nodules found in 4 to 7 percent of the adult U.S. population and solitary or multiple nodules found at much higher rates during ultrasonographic screening. "Most of these nodules — about 90 percent — are entirely benign," says Diana S. Dean, M.D., of the Division of Endocrinology, Diabetes, Metabolism, and Nutrition at Mayo Clinic in Rochester, Minn. "However, identifying the occasional thyroid cancer requires careful evaluation of every nodule we find, using a combination of clinical assessment, neck palpation, ultrasound imaging and, in many cases, analysis of a biopsy specimen."
Sometimes, thyroid nodules are noticed by the patient or a family member or are discovered during a routine physical examination. They rarely cause symptoms, unless they are large enough to interfere with swallowing. Thyroid cancer can invade and damage the recurrent laryngeal nerve, causing hoarseness. Such invasion and damage are infrequent.
"Most nodules are incidental discoveries," notes M. Regina Castro, M.D., of the Division of Endocrinology, Diabetes, Metabolism, and Nutrition at Mayo Clinic in Rochester, Minn., "and now many more such nodules are discovered because of the increased use of imaging performed for other reasons, including carotid ultrasonography, neck or chest computed tomography, magnetic resonance imaging, and even positron emission tomography."
"Diagnosing a thyroid nodule accurately and promptly is important," says Geoffrey B. Thompson, M.D., of the Department of Surgery at Mayo Clinic in Rochester, Minn., "because early diagnosis improves the likelihood that a cancer can be discovered while contained within the thyroid gland and amenable to surgery. Once soft tissue invasion has occurred or lymph nodes are extensively involved, the chance of surgical cure drops substantially, especially in older patients, and there is a much higher incidence of metastatic spread of these late-stage cancers."
"Prompt diagnosis is also important for the patient because the finding of a nodule often raises fears about cancer and a delay to diagnosis fuels the concern and anxiety," says John C. Morris III, M.D., of the Division of Endocrinology, Diabetes, Metabolism, and Nutrition at Mayo Clinic in Rochester, Minn. The most recent set of guidelines from the American Thyroid Association specifies that the evaluation of a thyroid nodule should include:
- Clinical assessment to determine the number, size and location of all nodules within the gland
- Measurement of serum thyrotropin (TSH) to exclude hyperthyroidism
- An ultrasound to assess the nodule for features of malignancy
- Fine-needle aspiration (FNA) of nodules that meet the appropriate size and ultrasound criteria
"However," Dr. Morris goes on to say, "not every nodule needs to be biopsied, so the clinical scenario and ultrasound features are important in selecting the appropriate nodule for biopsy. Typically, these steps involve several appointments for the patient and often take a number of days to weeks. To streamline the evaluation, we created the Thyroid Nodule Clinic, at which patients with thyroid nodules can have their assessment completed within a day or so."
Opened in July 2009, the Thyroid Nodule Clinic provides a one-stop thyroid nodule evaluation that includes a focused clinical assessment, ultrasound evaluation and FNA — all typically performed within a 60-minute appointment. "The ultrasound allows us to select both palpable and impalpable nodules for biopsy and target the most suspicious nodule, which is not always the largest nodule," says Dr. Dean. "Using ultrasound guidance for those biopsies, we have improved our diagnostic yield dramatically. We perform more than 800 biopsies every year in this way and can now expect a diagnosis in more than 95 percent of cases at the first attempt."
Furthermore, because of the coordinated assessment provided through the Thyroid Nodule Clinic, FNA cytology reports are typically available within two hours, so the patient usually receives a definitive result of the entire assessment within four hours. Patients with a benign thyroid nodule can be reassured, and those with a malignant or suspicious nodule can be offered an appropriate surgical referral, often within 24 hours. Dr. Dean concludes: "We believe that the Thyroid Nodule Clinic improves our care of these patients while lowering costs, improving efficiency and providing a better service to the referring physician."