诊断
为诊断脊索瘤,医疗护理专业人员可能会进行体格检查并询问您的健康史。其他检查和医疗程序可能包括影像学检查和采集组织样本进行实验室检测。
影像学检查,例如 CT 扫描或 MRI
影像学检查可以生成人体图像。从而能够显示癌症病灶的大小及部位。CT 扫描最适合观察骨骼变化。MRI 扫描更适合显示肿瘤及其周围组织。
- CT 扫描。 CT 扫描能够很好地显示骨骼变化,例如孔洞或薄弱点。在 CT 扫描中,脊索瘤通常表现为周围伴有骨质破坏的亮斑或暗斑。CT 扫描还可以显示肿瘤是否已扩散,例如颅骨和颈骨附近。有时,CT 扫描会使用一种被称为造影剂的特殊染料。这种染料在影像上显示更明亮。这样可以更好地显示所扫描的特定部位。
- MRI 扫描。 MRI 扫描能更好地显示肿瘤及其周围的血管。MRI 扫描可以显示肿瘤是否有不同的部分,以及它如何影响脊柱周围的组织。脊索瘤通常表现为内部有较暗区域的亮斑。
活检
活检是一项采集组织样本并在实验室中进行检测的医疗程序。活检对于确认影像学检查中所见是否为脊索瘤至关重要。这是因为在影像学扫描中,脊索瘤可能看起来像其他需要不同治疗的状况。对于脊索瘤,可能通过以下方式采集组织样本:
- 经皮肤插入一根针。 进行穿刺活检时,医务人员会将一根细针经皮肤插入,并将其引导至癌症部位。医务人员使用这根针来采集少量组织样本。某些脊索瘤(例如位于颅底者)可能无法在术前进行活检。
- 在手术期间取出样本。 进行手术活检时,外科医生会在皮肤上做一个切口,以触及癌变部位。外科医生取出一小块癌变组织进行检测。
医护团队需要仔细制定计划,确定应当如何进行活检。医护团队进行活检的方式需要留出余地,让将来仍能通过手术切除癌症。因此,最好前往接诊过许多脊索瘤患者的医疗中心就医。
为确认是脊索瘤,医护团队会寻找脊索瘤的病理体征。其中可能包括:
- 内部看起来有气泡的细胞,称为空泡细胞。
- 一种称为 brachyury 的特殊蛋白,常见于脊索瘤细胞中。
- 其他蛋白,例如 S100、波形蛋白和泛细胞角蛋白。
基因检测
脊索瘤的常规诊断不包括基因检测。但有时会建议有脊索瘤病史的家庭或者患有脊索瘤的儿童和年轻人进行基因检测。
治疗
脊索瘤治疗取决于肿瘤的大小和位置,以及是否侵入神经或其他组织。
- 手术通常是第一步,也是一种重要的脊索瘤治疗方法。在肿瘤能被完全切除的情况下,治愈的概率最大。
- 手术后通常会进行放射疗法,杀死可能残留的任何癌细胞。有时会在手术前使用放射疗法缩小肿瘤,使其更容易切除。有时,如果无法通过手术切除肿瘤,可能会单独使用放射疗法。
- 靶向治疗药物可用于已在体内扩散的癌症(称为转移瘤),或用于初始治疗后复发的癌症(即复发癌)。
在某些情况下,脊索瘤可以治愈。但脊索瘤可能很难治疗。它们很难被完全切除,因为它们的生长位置非常靠近脑和脊柱。而且常规的放射疗法和化疗对它们无效。脊索瘤常会再次出现。这被称为复发。如果发生这种情况,治疗可以帮助长期控制或管理癌症,但不是治愈。
手术
内镜颅底手术
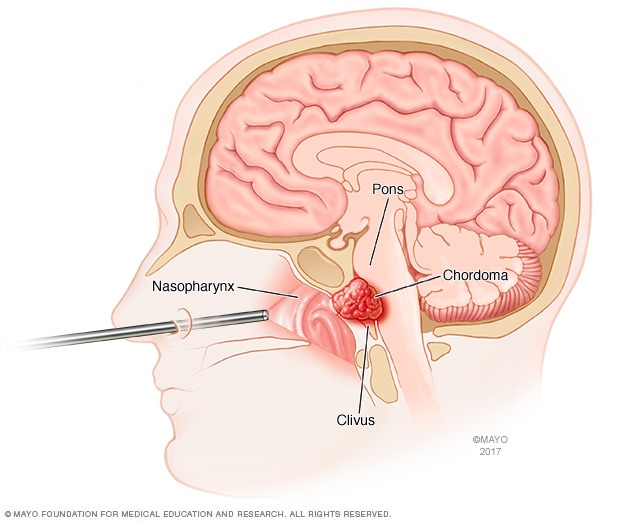
内镜颅底手术
内镜颅底手术使用一种被称为内镜的细长管进入颅底。内镜通过鼻子进入。外科医生通过内镜放入工具进行手术。本图显示使用内镜经鼻治疗脊索瘤,脊索瘤是一种通常发生于颅底的骨癌。
在脊索瘤手术中,外科医生的目标是尽量多地切除一整块肿瘤。在脊柱活动节段或骶骨中进行这种手术时,被称为整块切除术。如果能将脊索瘤整块完全切除,这种医疗程序可以降低癌细胞扩散和癌症复发的概率。
但要切除整个脊索瘤可能很困难。这是因为脊索瘤生长在重要结构(包括脑、脊髓、神经和血管)周围。外科医生尽力在不损伤健康结构的情况下切除癌变部位。安全到达颅底的某些部位也具有挑战性。
如果脊索瘤无法被完全切除,外科医生会尽量切除尽可能多的肿瘤。
手术类型可能因肿瘤位置而异:
- 颅底脊索瘤手术。 有时,外科医生可能通过鼻腔触及颅底脊索瘤。这种手术被称为内镜颅底手术。术中使用一根名为内镜的细长管。经鼻腔插入内镜,到达癌变部位。可以通过内镜送入专用工具,切除癌变部位。有时需要进行传统的开放手术。在开放手术期间,外科医生通过头部或颈部后方的一个大切口插入手术器械。也可能使用其他方法。
- 脊柱活动节段和骶骨脊索瘤手术。 对于颅底以下脊柱区域的脊索瘤手术,目标是尽可能多地切除肿瘤。周围的其他骨骼和组织也可能被切除。如果肿瘤位于脊柱底部的骶骨内,可能需要切除整个骶骨。这被称为骶骨切除术。该手术可通过腹部切口或背部切口进行。
极少数情况下,外科医生可能建议再做另一次手术来稳定原癌变部位。
脊索瘤手术的并发症包括任何手术都存在的风险,例如感染、血凝块和出血。如果手术过程中神经受损,也可能出现并发症。可能的并发症包括:
- 复视。
- 肠道或膀胱变化。
- 性功能丧失。
- 麻木感或感觉丧失。
- 行走或坐姿困难。
- 脑脊液(脑和脊髓周围的液体)泄漏。
放疗
放射疗法用高能能量束来治疗癌症。能量来自 X 线、光子、质子或其他来源。
进行放射疗法时,患者躺在治疗床上,一台机器围绕身体移动。机器向身体上的精确点位发送放射线。
过去,脊索瘤对标准放疗有抵抗性,需要以足够低的剂量进行放疗,才不会损害附近的任何脊髓或脑组织。较新的放射治疗方法可能有所帮助,它们能将更高剂量的放射更直接地递送到肿瘤,同时保护周围的脑、脊髓和神经。举例来说,放射方案包括:
所用的放射疗法类型可能因癌症所在位置和手术中心具备的方案而异。
放射疗法的副作用可能包括:
- 疲倦。
- 皮肤肿胀、刺激或其他变化。
- 头痛。
- 激素变化,例如垂体功能减退症。
- 脑部变化或损伤。
- 听力和视力变化。
- 难以吞咽。
放射疗法也存在轻微风险,可能会在以后导致其他癌症。这被称为继发性癌症。
靶向治疗药物
标准化疗通常不能使脊索瘤缩小。但是,癌症靶向治疗是一种使用药物攻击癌细胞中特定化学物质的治疗方法。通过阻断这些化学物质,靶向治疗可以使癌细胞死亡。
靶向治疗有时会作为临床试验的一部分使用。或是作为超说明书用法,治疗扩散到身体其他部位的脊索瘤(称为转移性脊索瘤)。超说明书用法表示药物已经获得美国食品药品管理局批准,用于治疗另外一种状况。治疗后复发的脊索瘤(称为复发性脊索瘤)也可以使用靶向治疗。
举例来说,一些可能首先用于脊索瘤的靶向治疗药物包括:
有时也可能使用其他药物。其中可能包括:
- 伊马替尼联合化疗药物或西罗莫司。
- 厄洛替尼。
- 拉帕替尼
- 索拉非尼。
靶向治疗的副作用可能包括:
- 疲倦。
- 胃部不适。
- 皮疹。
- 腹泻。
- 肿胀。
- 甲状腺和肾脏变化。
正在研究的治疗方法
科学家们持续研究脊索瘤的可能新治疗方法。其中包括:
- 检查点抑制剂。 这是一类有助于免疫系统发现和攻击癌细胞的药物。
- Brachyury 靶向治疗。 脊索瘤几乎总是会产生 brachyury 蛋白。因此,正在试验以 brachyury 为靶向的疫苗和新药。
临床试验
探索 Mayo Clinic 的研究 测试新的治疗、干预与检查方法,旨在预防、检测、治疗或控制这种疾病。
妥善处理与支持
随着时间的推移,您会找到合适的方法,帮您应对癌症诊断带来的不确定性和担忧。在此之前,以下措施可能有帮助:
充分了解脊索瘤以便作出治疗决策
请向医护团队咨询您所患癌症的情况,包括检查结果、治疗方案以及预后(如果您想知道)。您对您所患脊索瘤了解得越全面,就能越自信地作出治疗决定。
此外,辅助装置和设备可能有助于解决一些活动方面的问题。如果您有癌症疼痛,有一些治疗方法可供选择。您的治疗方案可能取决于导致癌症疼痛的原因以及感受到疼痛的严重程度。
与朋友、家人或社区保持密切联系
朋友、家人或社区资源可帮助提供您可能需要的实际支持。例如,他们可以在您住院期间帮您照顾家里。
与人交谈
寻找愿意听您诉说希望和担忧的倾听者。可以是您的朋友或家人。咨询师、医务社工、神职人员或者癌症互助组的关心和理解,可能也会对您有所帮助。
向医护团队咨询您所在地区的互助组。其他信息来源包括美国国家癌症研究所、美国癌症协会、脊索瘤基金会和妙佑医疗国际网联社区在线肉瘤互助组。脊索瘤基金会还提供脊索瘤专科医生名录。
准备您的预约
如有任何症状令您担心,请与医生或其他医疗护理专业人员约诊。如果医疗护理专业人员怀疑您患有脊索瘤,可能会将您转诊至专科医生,
由于就诊时间有限,因此最好提前做好准备。以下信息可以帮您做好准备。
您能做些什么
- 了解需要提前做的任何准备。 约诊时,请务必咨询是否需要提前做任何准备,例如限制饮食。
- 写下您目前具有的症状,包括看似与您约诊的原因无关的症状。
- 写下重要个人信息,包括重大压力或近期生活变化。
- 列出您正在使用的所有药物、维生素和补充剂及其剂量。
- 请家人或朋友陪同。 可能很难记住就诊时提供的所有信息。陪同者可能会记住您遗漏或遗忘的内容。
- 写下要向医疗护理团队咨询的问题。
由于向医疗护理团队咨询的时间有限,因此准备好问题清单有助于充分利用就诊时间。请按照重要程度从高到低的顺序列出问题,以免时间不够。对于脊索瘤,要咨询的一些基本问题包括:
- 我是否患有脊索瘤?
- 脊索瘤处于哪个分期?
- 脊索瘤是否已经扩散到身体其他部位?
- 我是否需要做更多检查?
- 有哪些可选的治疗方案?
- 每种治疗方法分别能多大程度上增加治愈几率或延长寿命?
- 每种治疗方法都有哪些潜在的副作用?
- 每种治疗方法对我的日常生活有何影响?
- 有没有一种治疗方案您认为最适合我?
- 就我这种情况,您对我的朋友或家人有什么建议?
- 我是否应该去看专科医生?
- 有没有我可以带走的手册或其他印刷材料? 您推荐哪些网站?
- 哪些因素决定我是否应该制定复诊计划?
如果还有其他问题,请随时提出。
医生可能会做什么
请准备好回答相关问题,例如:
- 您何时开始出现症状?
- 您的症状是持续存在,还是偶尔出现?
- 您的症状有多严重?
- 有没有什么因素似乎会改善您的症状?
- 有没有什么因素似乎会加重您的症状?
Oct. 17, 2025