Sept. 24, 2019
The sacroiliac (SI) joint is a common but underrecognized source of continuing back pain in patients who have surgical fusions for the treatment of back pain. Mayo Clinic has developed new techniques for the diagnosis and treatment of patients with SI joint dysfunction.
"The SI joint is often glossed over as a pain generator, especially in people who have had spinal fusion and experience continued pain," says William W. Cross III, M.D., an orthopedic surgeon at Mayo Clinic in Rochester, Minnesota. "As with joints involved in cranial adjacent segment disease, the SI joint can respond adversely to the increased forces. In our clinic we routinely see patients who have had one, two or even three spinal fusions but develop or continue to have SI joint pain."
Research has established that the SI joint is the source of pain in nearly half of patients who experience new or continued low back pain after fusion surgery. Dr. Cross notes that SI joints normally move less than 1 millimeter. "But with force transfer after spinal fusion, the SI joints can move a couple of millimeters," he says. "For some patients, that's exquisitely painful."
Persistent abnormal motion in the SI joint can lead to premature degenerative changes. "We have seen patients ranging in age from their mid-30s to their 80s who have had degenerative changes in the SI joint after spinal fusion," Dr. Cross says. "This is not just age-related degeneration. Anybody who has fusion surgery can develop SI dysfunction. It is important to note, however, that the absence of degenerative changes in the SI joint does not eliminate the SI joint as a potential pain generator."
Finding and fixing the source of pain
Differing presentations of severe sacroiliac joint pain
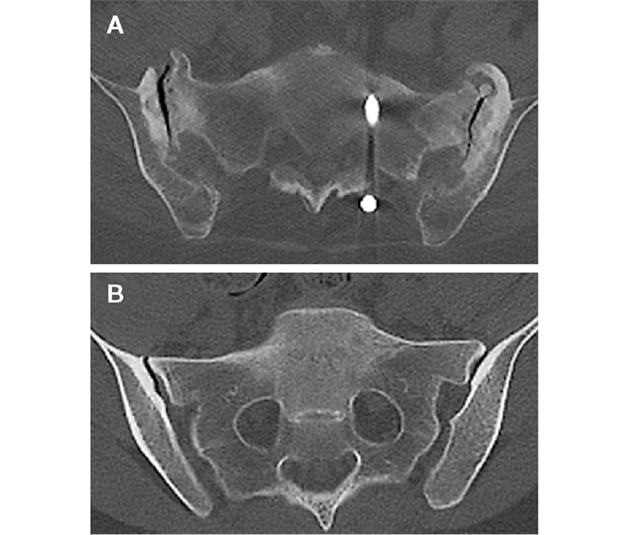
Differing presentations of severe sacroiliac joint pain
Axial CT images illustrate two differing presentations of severe sacroiliac (SI) joint pain. A. Image shows significant SI joint degenerative changes secondary to chronic pelvic instability from pubic symphysis resection 30 years earlier. B. Image shows no significant joint degeneration.
The diagnosis of SI joint dysfunction requires an extensive patient history and comprehensive physical examination. "No single test can perfectly diagnose the condition," Dr. Cross says. "The imaging can look normal, and the reliability of common physical exam techniques can be poor."
Mayo Clinic's physical evaluation combines the flexion, abduction and external rotation (FABER) test and a posterior superior iliac spine (PSIS) distraction test. "The maneuver, what I have termed the Mayo SI test, manipulates the SI joint in such a way that it can cause extreme pain in some patients," Dr. Cross says. "It is interesting to note that this test is often normal during postoperative follow-up, making it a great marker for diagnosis and successful treatment."
First line treatment for SI joint dysfunction consists of nonoperative management, such as physical therapy, an SI joint belt, injections and anti-inflammatory medication. SI joint fusion surgery is considered only after those options have been exhausted.
"If there's no hardware in or across the SI joint from a previous surgery, a steroid might give some durable pain relief," Dr. Cross says. "However, if the steroid doesn't work and SI fusion is anticipated, we wait three months because of the potential increased risk of infection with steroid use."
Unilateral sacroiliac fusion procedure
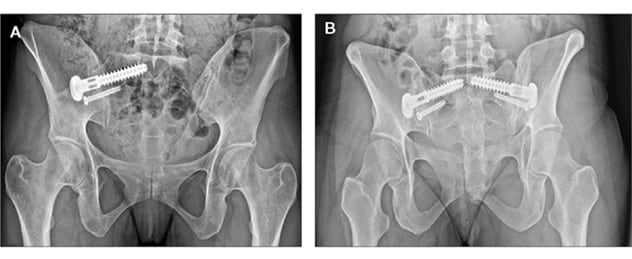
Unilateral sacroiliac fusion procedure
A. Image illustrates unilateral sacroiliac (SI) fusion procedure using a system that provides a principles-based fusion, maximizing the concepts of joint preparation, compression and stability. B. Image illustrates a bilateral SI fusion procedure using the same system.
When surgery is indicated, Mayo Clinic uses a new, minimally invasive SI fusion implant developed by researchers at Mayo Clinic and CoorsTek Medical and approved by the Food and Drug Administration. The device entered clinical use in late 2017.
So far, the outcomes are promising. Measured with the visual analog of subjective pain assessment, patients' pain scores decline by roughly five points after implantation of the new device. Average scores on the single assessment numeric evaluation (SANE) exam are 80%, 91% and 96% at eight weeks, six months and 12 months after surgery, respectively.
The SI fusion system follows the principles of arthrodesis: aggressive joint preparation, enhanced compression and stability. "We designed this system because we think no other system fits the true philosophy of how the SI joint should be fused," Dr. Cross says. "SI joint fusion should be no different from any other fusion surgery. You have to employ these principles to achieve durable, long-term outcomes that are going to return patients to a much greater quality of a life."