April 08, 2016
Although there is general agreement that patients with a previous history of a hip or vertebral fracture or those with bone mineral density (BMD) T-scores less than or equal to -2.5 at the femoral neck, total hip or lumbar spine by dual energy X-ray absorptiometry (DXA) warrant initiation of drug therapy for osteoporosis, it is clear that approximately 60 percent of fragility fractures in women and approximately 80 percent of fragility fractures in men occur in patients with T-scores above this value.
Not surprisingly, clinicians often see patients with T-scores above -2.5 who have had fragility fractures, leading to uncertainty as to the true extent of skeletal fragility present in these patients. Thus, there is a critical need for novel approaches to better identify patients with osteopenia (T-scores -2.5 to -1) who may be at increased fracture risk.
Over the past decade, a unique partnership involving the clinical research expertise of Sundeep Khosla, M.D., and colleagues at Mayo Clinic and the bioengineering capabilities of Tony M. Keaveny, Ph.D., and his group at the University of California, Berkeley has contributed to the development of one such approach.
Dr. Khosla, an endocrinologist at Mayo Clinic in Rochester, Minnesota, explains: "This technology, VirtuOst, is now commercialized by O.N. Diagnostics, a company started by Dr. Keaveny. VirtuOst, which has been cleared by the Food and Drug Administration, utilizes clinical computerized tomography (CT) scans that may have been obtained for any purpose (such as standard abdominal imaging or CT colonography) to obtain noninvasive measures of bone strength using finite element analysis (FEA). These bone strength measures at the spine or hip are highly correlated with the true breaking strength of bone in cadaveric studies.
Process by which CT images are analyzed
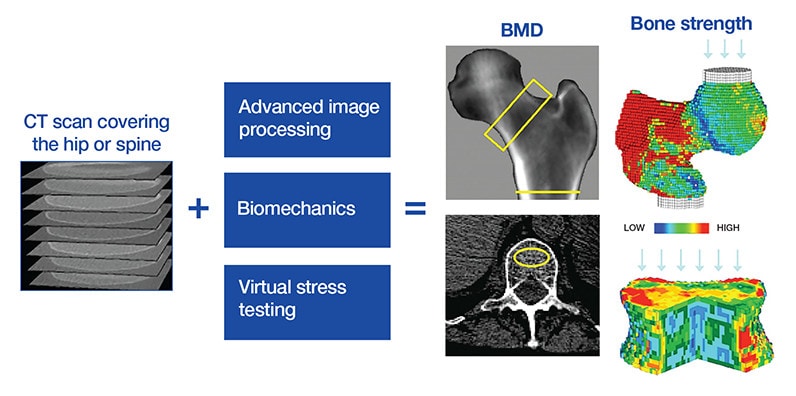
Process by which CT images are analyzed
The overall test provides measures of a DXA-equivalent bone mineral density (BMD) at the hip and trabecular BMD at the spine, and measures of bone strength at both sites. The input CT scan is processed to separate out the bones of interest to measure BMD. The same bones are then converted into engineering finite element models for virtual stress testing, using information on the biomechanical behavior of bone tissue and its relation to bone density from the CT scan. Strength measurements are computed for the femur in a sideways-fall configuration and for the spine for a compressive overload.
"The figure depicts the process by which CT images are analyzed. Based on the empirical relationship between CT density and the yield stress of bone, FEA is used to virtually load the bone to failure, thereby arriving at the FEA-based bone strength, in units of newtons (N)."
The use of FEA-derived bone strength at the spine or the hip has now been validated in a number of retrospective and prospective fracture-outcome studies whose outcomes were published in Radiology in 2016, American Journal of Gastroenterology in 2014, Osteoporosis International in 2012 and Journal of Bone and Mineral Research in 2010. Based on these studies, thresholds for fragile bone strength at the spine or the hip, separately in women and in men, have been derived.
Dr. Khosla highlights: "Collectively, these studies have demonstrated that using these thresholds, virtually all patients who fracture with BMD-defined osteoporosis are accurately identified. Moreover, these thresholds also identify a significant number of patients with fragility fractures who have osteopenia, demonstrating that the FEA-derived bone strength is capturing aspects of bone structure and strength not evident by conventional DXA.
"To identify osteoporosis, this analysis provides a measurement of trabecular BMD at the spine that avoids artifacts inherent in DXA due to degenerative changes or aortic calcification; it also provides DXA-equivalent measurements of total hip and femoral neck BMD T-scores at the hip that are highly correlated with DXA.
"Recently, the International Society for Clinical Densitometry has endorsed these BMD and bone strength measurements, and their validated thresholds, as a sufficient basis for identifying patients for initiation of pharmacological therapy."
The Metabolic Bone Group at Mayo Clinic has gained experience in using FEA-derived bone strength as part of its practice in specific groups of patients. These uses include:
- Patients undergoing CT imaging for other purposes, for which the bone strength analysis can be an add-on, providing additional information regarding skeletal fragility. If the imaging includes the proximal femur, a DXA-equivalent T-score also is obtained.
- Patients with fragility fractures in the setting of a DXA BMD T-score of greater than -2.5. For these patients, a CT scan specifically for bone strength analysis can be obtained and the images processed for spine and hipbone strength. A finding of bone strength in the fragile range, despite a BMD by DXA that is not considered osteoporotic, can provide an explanation for the patient's fragility fractures.
Dr. Khosla says: "As we gain more experience with this technology, bone strength analyses from CT imaging may prove to be useful in patients with osteopenia who have not yet fractured, but where fracture risk based on FRAX or other criteria appear to be increased or remain ambiguous. A subset of these patients may have compromised bone strength and thereby warrant consideration for drug therapy.
"Moreover, as we learn more about how bone strength and, in particular, the distribution of bone within the spine or hip change with various therapies for osteoporosis, this approach also may become useful in determining the best choice of therapy for particular patients with very low bone strength and perhaps for monitoring response to therapy. To the extent that certain medications may replace bone precisely where it is needed to maximize bone strength, we may be able to identify optimal responses to pharmacological therapy."
Dr. Khosla concludes: "Obtaining an FEA-derived bone strength may be useful in the clinical evaluation and management of patients at risk of fractures. After over a decade of collaboration between Mayo Clinic and the University of California, Berkeley, this technology is now clinically available. For selected patients, it could greatly enhance fracture risk stratification."
For more information
Fidler JL, et al. Comprehensive assessment of osteoporosis and bone fragility with CT colonography. Radiology. 2016;278:172.
Weber NK, et al. Validation of a CT-derived method for osteoporosis screening in IBD patients undergoing contrast-enhanced CT enterography. American Journal of Gastroenterology. 2014;109:401.
Srinivasan B, et al. Relationship of femoral neck areal bone mineral density to volumetric bone mineral density, bone size, and femoral strength in men and women. Osteoporosis International. 2012;23:155.
Melton LJ III, et al. Relation of vertebral deformities to bone density, structure, and strength. Journal of Bone and Mineral Research. 2010;25:1922.