July 20, 2021
Fuchs' endothelial corneal dystrophy (FECD) is a highly prevalent, bilateral, late-onset heritable disorder that affects the corneal endothelium. FECD is also the most common trinucleotide repeat expansion disorder.
"Many patients with FECD harbor an intronic cytosine-thymine-guanine, or CTG, trinucleotide repeat expansion in the transcription factor 4 gene on chromosome 18 — also termed CTG18.1 expansion. CTG repeat lengths are typically 12 to 30 repeats long. Repeat lengths greater than 40 are pathogenic, causing FECD," says Keith H. Baratz, M.D., a consultant in Ophthalmology at Mayo Clinic in Rochester, Minnesota.
Dr. Baratz and fellow researchers collaborated to describe the clinical and genetic variables in a large cohort of unrelated subjects with and without FECD, as well as in a cohort of families affected by FECD with and without CTG18.1 expansion. The researchers also sought to characterize the modes of inheritance of FECD, intergenerational CTG18.1 expansion length stability, phenotypic penetrance and sex differences. Their findings were published in Investigative Ophthalmology & Visual Science in 2021.
The cohort
From June 1, 2007, through Aug. 1, 2019, clinician-investigators recruited 1,000 subjects, including patients with FECD and their family members and patients 50 years or older without FECD who served as control subjects. Subjects who initially sought ophthalmic care for FECD were defined as probands.
The clinical hallmark of FECD is excrescence of Descemet's membrane (guttae). FECD cases were defined as subjects having excrescence with a Krachmer grade of 2 or more (more than 12 scattered, nonconfluent guttae). Controls were defined as subjects having excrescence with a Krachmer grade 0 (no guttae) or grade 1 (12 or fewer scattered, nonconfluent guttae). Grades 2 to 4 were defined as mild FECD, and grades 5 to 6 were defined as severe FECD. There were 546 unrelated cases of FECD (67.6% female) and 235 controls (63.8% female) in the cohort.
Representative pedigrees of families affected by FECD
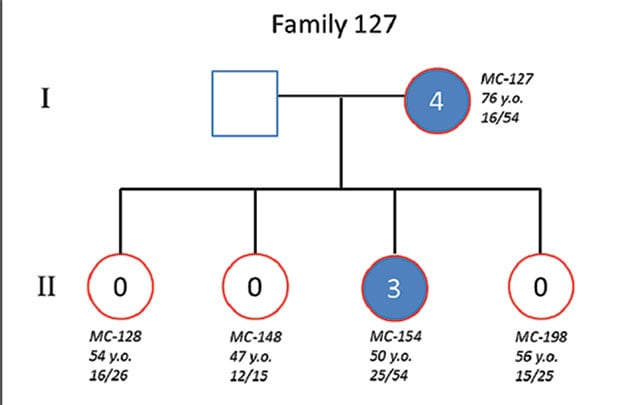
Representative pedigrees of families affected by FECD
Researchers compared descriptive statistics between affected and unaffected subjects with FECD and between father and mother transmission, reporting the following:
- CTG18.1 expansion (repeats greater than 40 CTG trinucleotides) was observed in 424 (77.7%) cases and 18 (7.7%) controls (P = 2.48 × 10-44).
- CTG18.1 expansion was associated with FECD severity (P = 5.62 × 10-7).
- The family arm included 331 members from 112 families affected by FECD; 87 families showed CTG18.1 expansion.
- Autosomal dominant inheritance with variable expression of FECD was observed regardless of expansion status.
- FECD penetrance of CTG18.1 expansion increased with age, but even in the oldest age quartile (64 to 91 years) penetrance was incomplete at 86%.
- Instability of the repeat length, which is common in other repeat expansion diseases such as Huntington's disease and myotonic dystrophy, was assessed in 62 parent-offspring transmissions of CTG18.1 expansion. Forty-eight (77.4%) subjects showed minimal instability in CTG18.1 repeat length of 10 or fewer; eight (12.9%) had a change of 50 or more repeats, including five large expansions (approximately 1,000 to 2,000 repeats) that contracted.
"Very surprisingly, among 44 offspring who did not inherit the CTG18.1 expansion allele, eight (18.2%) still exhibited FECD," says Dr. Baratz.
The effect of sex, CTG18.1 expansion status and CTG18.1 repeat length on FECD severity was also assessed, with the following results:
- After age adjustment, sex was not associated with FECD severity (P = 0.69). Compared with mild FECD cases, severe FECD cases were more often positive for CTG18.1 expansion and had on average greater CTG18.1 repeat length.
- After age and sex adjustment, CTG18.1 expansion status remained significantly associated with FECD severity (P = 5.62 × 10-7).
- Severe FECD was also associated with CTG18.1 repeat length among all FECD cases (P = 8.8 × 10-4), but FECD severity was not associated with CTG18.1 repeat length when examining only FECD cases with CTG18.1 expansion (P = 0.33).
Dr. Baratz notes: "Results of this large-cohort study confirm the presence of CTG18.1 expansion in a large proportion of FECD cases, at least in this predominantly white U.S. patient group. This finding contrasts with findings by us and others that CTG repeat expansion accounts for a minority of cases in other racial and ethnic groups, and the primary cause of FECD in other populations remains an important question.
"Novel findings include the assessment of phenotypic penetrance of CTG18.1 expansion, the lack of a clear pattern of intergenerational contraction or expansion of CTG18.1 expansion, and the surprisingly common occurrence of the FECD phenotype in family members who do not harbor the CTG18.1 expansion but are part of families with CTG18.1 expansion. These observations highlight the complex relationship between FECD and the repeat expansion and emphasize the gaps in knowledge regarding other genetic and environmental factors influencing the penetrance and expression of FECD."
For more information
Xu TT, et al. Disease expression and familial transmission of Fuchs endothelial corneal dystrophy with and without CTG18.1 expansion. Investigative Ophthalmology & Visual Science. 2021;62:17.