Diagnosis
Peutz-Jeghers syndrome (PJS) can be diagnosed based on a person's symptoms, medical history and family history and, sometimes, test results.
How Peutz-Jeghers syndrome is diagnosed
You can be diagnosed with PJS if you have any of the following:
- Two or more hamartomatous polyps in the digestive tract.
- Dark spots on the skin around or inside the mouth or on the genitalia, hands or feet combined with a family history of PJS.
- Any number of hamartomatous polyps when combined with a family history of PJS or with the presence of characteristic dark spots on the skin.
- A genetic test that shows a certain change, called a pathogenic or likely pathogenic change, in the STK11 gene.
Tests to screen for polyps and cancer
Colonoscopy exam
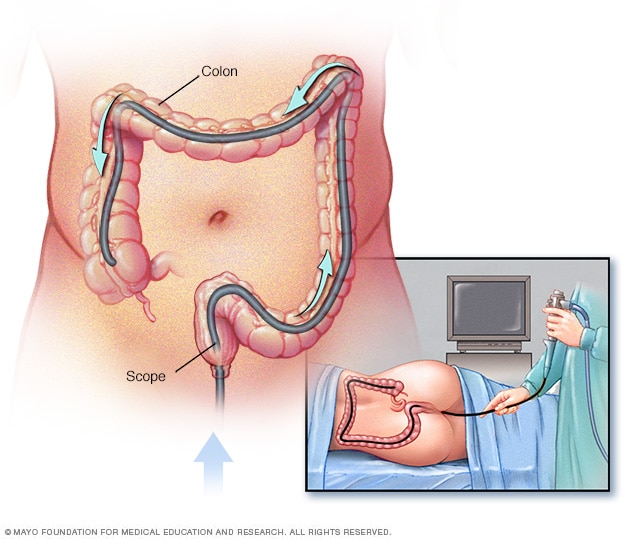
Colonoscopy exam
During a colonoscopy, a healthcare professional puts a colonoscope into the rectum to check the entire colon.
Endoscopy
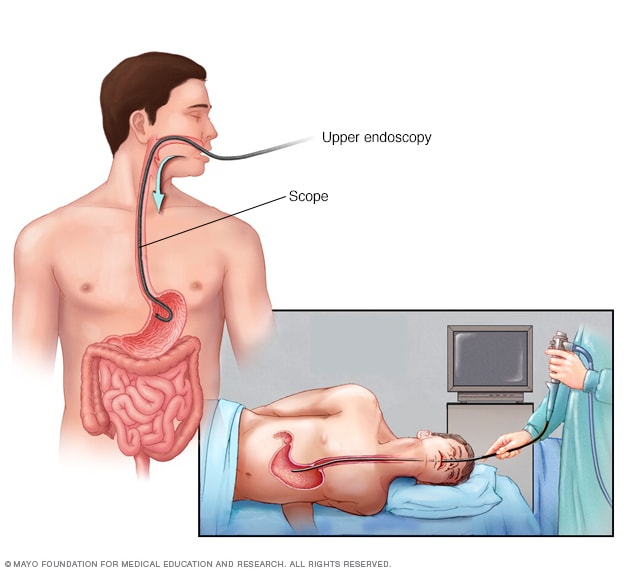
Endoscopy
An endoscopy procedure involves inserting a long, flexible tube called an endoscope down your throat and into your esophagus. A tiny camera on the end of the endoscope allows views of your esophagus, stomach and the beginning of your small intestine, called the duodenum.
Capsule endoscopy camera
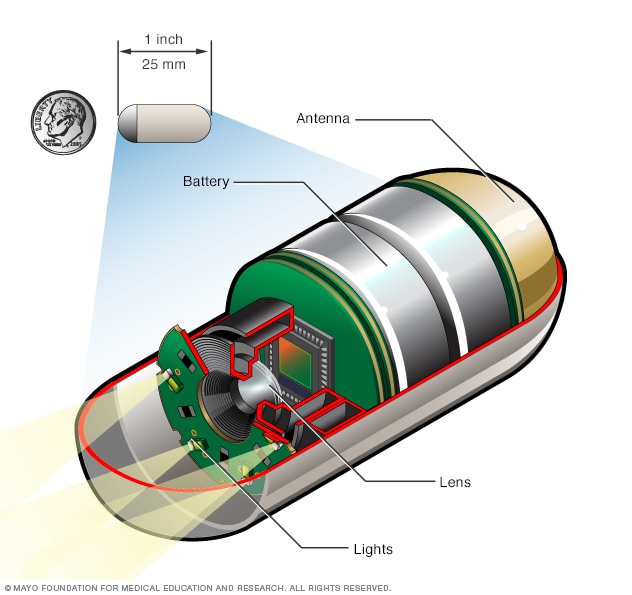
Capsule endoscopy camera
During a capsule endoscopy procedure, you swallow a tiny camera that's about the size of a large vitamin pill. The capsule contains lights to illuminate your digestive system, a camera to take images and an antenna that sends those images to a recorder you wear on a belt.
To help make the diagnosis and look for polyps and cancer, healthcare professionals sometimes use tests that look directly at the digestive tract. These tests may include:
- Colonoscopy. In this test, a small tube with a light and camera is inserted through the rectum to examine the entire colon. The tube is guided through the colon using air to distend the colon and to get a clear view. Images of the lining of the colon are shown in real time on a video screen. Polyps usually appear as bumps or slightly raised spots or patches on an otherwise smooth lining. If polyps are found, a healthcare professional may use tools inserted through the tube to take out the polyps or take tissue samples to send to a lab for analysis. There also is the possibility of finding other areas of concern in the colon that can be sampled at the time of the exam.
- Upper endoscopy. In this test, a healthcare professional uses a long, narrow tube called an endoscope through your mouth down the esophagus, stomach and upper part of the small intestine. The tube contains a light and a tiny camera to view these areas. If polyps are found, they can be fully or partly removed using tools inserted through the tube.
- Capsule endoscopy. In this test, you swallow a vitamin-sized capsule with a tiny wireless camera and lights inside it. The camera takes pictures as it moves through the digestive tract. This includes areas of the small intestine that a standard endoscope cannot reach. Usually, the capsule leaves the body in a bowel movement within a few days.
- Balloon-assisted enteroscopy. During this procedure, a scope and an overtube with one or two attached balloons are inserted through your mouth or anus into your digestive tract. This method allows your healthcare professional to see areas of the small intestine that a regular endoscope cannot reach. This test may be done to closely examine polyps seen on other tests and, in some cases, remove them.
- Lab tests. If polyps are found during any of these tests, they often are fully or partly removed. A medical professional who studies tissue samples, called a pathologist, looks at the polyp tissue under a microscope to find out what type of polyp it is. This helps confirm whether the polyps match those usually caused by PJS.
If a capsule endoscopy cannot be done, a healthcare professional may suggest an imaging test to view polyps in areas of the small intestine that can't be reached with a regular endoscope. These could include:
- Magnetic resonance imaging (MRI). This technique uses a magnetic field and computer-generated radio waves to create detailed images of the organs and tissues in the body. Most MRI machines are large, tube-shaped magnets. When you lie inside an MRI machine, the magnetic field inside works with radio waves and hydrogen atoms in your body to create cross-sectional images — like slices in a loaf of bread. The MRI machine also can produce 3D images that can be viewed from different angles. You are not getting radiation when you have an MRI.
- Magnetic resonance (MR) enterography. This test works in a manner that is similar to an MRI. But you also drink a contrast fluid before the exam. And at different times during the exam, you get injections of contrast and glucagon through a tube inserted into a vein, called an IV line. The contrast fluid helps make certain details on the images clearer.The glucagon is a medicine that slows the motion of the small intestine. This helps improve the image quality. You are not getting radiation when you have an MR enterography.
- Computerized tomography (CT) scan. You may have a CT scan — a special X-ray technique that provides more detail than a standard X-ray does. This test looks at the entire intestine as well as tissues outside it. CT enterography is a special CT scan that provides better images of the small intestine. You are getting a small dose of radiation during a CT scan.
Genetic testing
Genetic testing looks for a specific change in the STK11 gene using a blood sample. Finding this change can confirm a diagnosis of PJS. However, if you don't have the gene change, it doesn't rule out PJS. Some people with PJS do not have the gene change. In those people, the diagnosis can be based on the features of the polyps, the presence of the typical skin freckling pattern around the mouth, genitals, hands and feet, or a family history of PJS. If a gene change is found, genetic testing may be recommended for family members. This can allow for early treatment to help prevent complications.
Ongoing screening
Transvaginal ultrasound
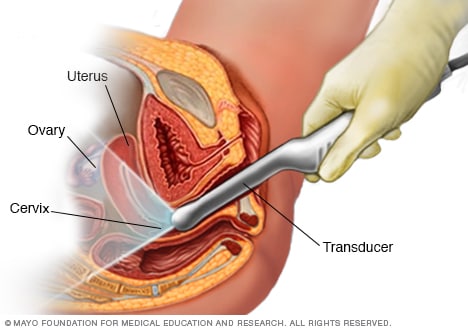
Transvaginal ultrasound
During a transvaginal ultrasound, a healthcare professional or technician uses a wandlike device called a transducer. The transducer is inserted into your vagina while you lie on your back on an exam table. The transducer emits sound waves that generate images of your pelvic organs.
Once a person is diagnosed with PJS, it's common to have some regular tests to check for polyps, cancer and other complications. If polyps are found, they may be removed during the procedure.
Which screening tests and how often they're done depends on your age, sex and personal history. Some of the tests are the same ones used to diagnose PJS. Screening tests may include the following:
- Colonoscopy and upper endoscopy, often starting between ages 8 and 10. These tests are used to check for polyps in the colon and stomach. The tests may be done earlier if you have symptoms. If no polyps are found, testing may start again at age 18. If polyps are found, or after the age of 18, these tests may be done every 2 to 3 years. Sometimes the tests are done more often.
- Capsule endoscopy or MR or CT enterography, often starting between ages 8 and 10. These tests are done to check for polyps in the small intestine. The tests may be done earlier if you have symptoms. If polyps are found, or after the age of 18, these tests may be done every 2 to 3 years. Sometimes the tests are done more often.
- A physical exam, usually starting at age 8 or when diagnosed in girls. These are done once a year to check for signs of early puberty. A blood test also can check for iron deficiency anemia, which can be a sign of bleeding polyps.
- A physical exam, usually starting at ages 8 to 10 in boys. These are done once a year to check the testicles for signs of tumors and the body for breast growth called gynecomastia. The breast growth can be caused by a type of tumor in the testicles. A blood test also can check for iron deficiency anemia, which can be a sign of bleeding polyps.
- A pelvic exam, pap smear and transvaginal ultrasound, often starting around ages 18 to 20 in women. These tests are done once a year to check for cervical, ovarian and uterine cancers.
- A clinical breast exam, mammogram and breast MRI, often starting around age 30 in women. Breast exams are needed every 6 to 12 months. Mammography and a breast MRI are needed once a year.
- MRI, MR cholangiopancreatography or endoscopic ultrasound, usually starting around age 30. One or more of these tests may be done to check for pancreatic cancer once a year. MR cholangiopancreatography is a special type of magnetic resonance imaging used to view the pancreas.
Conditions with similar symptoms
When diagnosing Peutz-Jeghers syndrome, healthcare professionals may consider other inherited conditions that can cause digestive tract polyps or skin changes.
Usually genetic testing can help make the diagnosis clear. But when the genetic testing results are not clear, some of these other conditions are considered. All are caused by different gene changes and affect the body in different ways.
- Juvenile polyposis syndrome. When comparing Peutz-Jeghers syndrome vs juvenile polyposis syndrome, both conditions can cause multiple hamartomatous polyps in the digestive tract and increase the risk of cancer. A key difference is that juvenile polyposis syndrome does not cause the dark spots in and outside the mouth and on the genitals, hands and feet that PJS does. Juvenile polyposis syndrome is linked to changes in genes other than the STK11 gene change that causes Peutz-Jeghers. These include changes in BMPR1A and SMAD4.
- Familial adenomatous polyposis (FAP). When comparing Peutz-Jeghers syndrome vs FAP, both involve digestive tract polyps and can lead to cancer. But FAP most often causes many adenomatous polyps in the large intestine. PJS causes mainly hamartomatous polyps that can appear throughout the digestive tract. FAP also does not cause dark spots on the skin, which are common with PJS. FAP is caused by changes in the APC gene, not STK11.
- Hereditary hemorrhagic telangiectasia, also called Osler-Weber-Rendu syndrome. When comparing Peutz-Jeghers syndrome vs hereditary hemorrhagic telangiectasia (HHT), they are different inherited conditions but can happen together in about 20% of people with PJS. HHT does not cause polyps like PJS does. But both conditions can cause skin symptoms. HHT can cause lacy red vessels or tiny red spots, mostly on the lips, face, fingertips, tongue and inside the mouth. These are called telangiectasias. HHT also often causes nosebleeds. HHT usually happens from changes in the ENG gene or ACVRL, not STK11.
These conditions are not the same as Peutz-Jeghers syndrome, even though some symptoms are similar.
Treatment
There is no cure for Peutz-Jeghers syndrome. PJS treatment focuses on screening for and managing polyps, cancer and other complications over time.
Peutz-Jeghers syndrome may be treated with:
- Polypectomy. During upper endoscopy, colonoscopy and balloon-assisted enteroscopy, polyps can be taken out in a process called polypectomy. Very small polyps might be taken out with forceps. Small to medium polyps often are taken out with a wire loop called a snare. Sometimes an electric current is applied to cut a polyp and prevent bleeding. Removing polyps helps prevent complications, such as bleeding, blocking of the intestine and intussusception.
- Surgery. Polyps that are too large to be removed safely with polypectomy are removed surgically. Surgery may be used for intussusception and polyps that block the intestine or that cause bleeding that can't be controlled with polypectomy. Surgery also may be needed if cancer is found.
- Managing anemia. Blood tests are used to check for iron deficiency anemia, which can happen when polyps bleed over time. If anemia is found, treatment is to identify and stop the source of the bleeding, such as removing bleeding polyps. Supportive care may be needed if you lose a lot of blood. For example, you might need fluids through a needle in a vein and possibly blood transfusions. Your healthcare professional also may prescribe iron.
- Cancer treatments. Cancers caused by PJS are treated the same as cancer in someone without PJS.
The life expectancy for Peutz-Jeghers syndrome varies. A person with PJS has between a roughly 40% and 93% risk of developing cancer at some point during life. The risk increases with age. The goal of treatment is to find and treat cancer early, when it might be more successful, as well as reduce symptoms and prevent other complications.
Clinical trials
Explore Mayo Clinic studies testing new treatments, interventions and tests as a means to prevent, detect, treat or manage this condition.
Preparing for your appointment
What you can do
Your time with your healthcare professional may be limited. It may help to prepare a list of questions ahead of time. For Peutz-Jeghers syndrome, some basic questions to ask may include:
- What are the chances that I will pass the condition on to my children or that my child will pass this condition on to any future children?
- What is the risk of cancer?
- How can I lower the risk of cancer?
- How often do I need screening tests?
- What kind of screening tests?
- How many polyps have been found and what kind?
- Will I need surgery?
- If I need surgery, when will I need it?
- What kind of surgery do I need?
- What kind of follow-up and treatment do I need?
- How accurate is genetic testing?
- Should my family members be tested for PJS?
Feb. 21, 2026