نظرة عامة
سرطان البروستاتا
سرطان البروستاتا
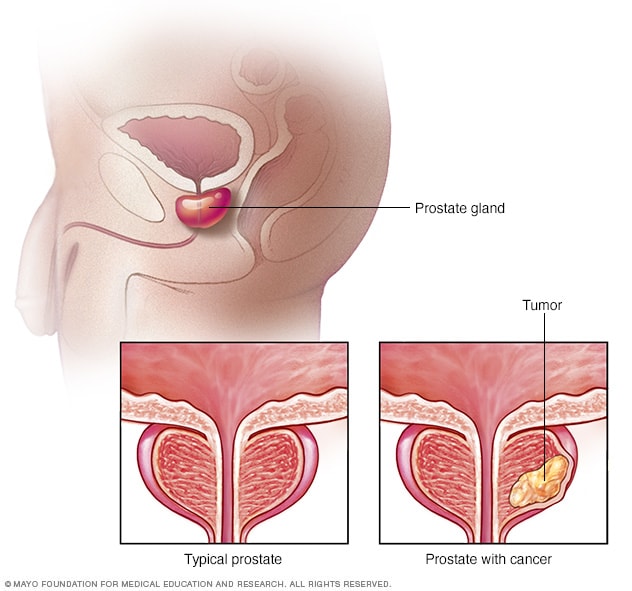
ينتج سرطان البروستاتا عن نمو خلايا سرطانية في البروستاتا. والبروستاتا غدة صغيرة تساعد في إنتاج السائل المنوي؛ فهي جزء من الجهاز التناسلي الذكري. يبين هذا الرسم التوضيحي غدة بروستاتا سليمة وغدة بروستاتا مصابة بالسرطان.
العلاج الهرموني لسرطان البروستاتا هو العلاج الذي يمنع إنتاج هرمون التستوستيرون أو يمنع وصوله إلى خلايا سرطان البروستاتا.
تعتمِد معظم خلايا سرطان البروستاتا على هرمون التستوستيرون للنمو. ويؤدي العلاج الهرموني إلى موت خلايا سرطان البروستاتا أو نموها ببطء.
قد يشمل العلاج الهرموني لسرطان البروستاتا تناوُل الأدوية أو حتى إجراء عملية جراحية لاستئصال الخِصيتين.
يُعرَف العلاج الهرموني لسرطان البروستاتا أيضًا بعلاج الحرمان من الأندروجين.
Types
Types of hormone therapy for prostate cancer include:
- Medicines that stop the body from making testosterone. Some medicines block signals that tell the testicles to make testosterone. These medicines are called luteinizing hormone-releasing hormone (LHRH) agonists and antagonists. Another name for them is gonadotropin-releasing hormone (GnRH) agonists and antagonists.
- Medicines that block the action of testosterone in the body. These medicines are known as antiandrogens. They're often used with LHRH agonists. That's because LHRH agonists can cause a brief rise in testosterone levels before testosterone levels go down.
- Surgery to remove the testicles. This surgery is called an orchiectomy. It lowers testosterone levels in the body quickly. In some cases, only the part of the testicles that makes testosterone is removed. Both procedures are permanent.
In the form of medicine, hormone therapy for prostate cancer, also called ADT, can be given all the time or off and on:
- Continuous ADT is given without stopping.
- Intermittent ADT is given for a set amount of time or until a prostate-specific antigen (PSA) test shows a low number. This test measures a protein produced by both cancerous and noncancerous tissue in the prostate. If the number is low, the treatment is paused. If the cancer comes back or gets worse, the treatment may start again.
Some early studies show that intermittent ADT may cause fewer side effects and still work just as well as continuous ADT for some people. It also might help them feel better day to day.
المنتجات والخدمات
لماذا يتم إجراء ذلك
يهدف العلاج الهرموني لسرطان البروستاتا إلى منع إنتاج هرمون التستوستيرون في الجسم. فالتستوستيرون يساعد في نمو خلايا سرطان البروستاتا.
وقد يكون العلاج الهرموني لسرطان البروستاتا خيارًا مناسبًا في أوقات مختلفة ولأسباب متنوعة أثناء علاج السرطان.
يمكن استخدام العلاج الهرموني في الحالات التالية:
- لعلاج سرطان البروستاتا الذي انتشر في الجسم، والذي يُعرَف بسرطان البروستاتا النقيلي، عن طريق تقليص السرطان وإبطاء نمو الأورام. وقد يخفف العلاج أيضًا من الأعراض.
- بعد علاج سرطان البروستاتا، إذا كان مستوى المستضد النوعي للبروستاتا (PSA) لا يزال مرتفعًا أو يبدأ في الارتفاع.
- في حال سرطان البروستاتا الموضعي المتقدم للاستفادة من العلاج بالحزم الإشعاعية الخارجية في تقليل احتمال عودة السرطان للجسم مرة أخرى.
- لتقليل احتمال عودة السرطان إلى جسم المصابين الذين يرتفع احتمال تكرار إصابتهم بالسرطان.
المخاطر
قد تشمل الآثار الجانبية للعلاج الهرموني لسرطان البروستاتا ما يلي:
- نقص الكتلة العضلية
- زيادة دهون الجسم
- فقدان الدافع الجنسي
- عدم القدرة على الانتصاب أو الحفاظ عليه، وهو ما يُعرَف بضعف الانتصاب
- ترقُّق العظام، الذي قد يؤدي إلى كسر بالعظام
- هبات الحرارة
- قلَّة شعر الجسم وصِغَر الأعضاء التناسلية ونمو أنسجة الثدي
- الشعور بالتعب
- مرض السكري
- أمراض القلب
كيف تستعد
إذا كنت تفكر في تلقي العلاج الهرموني لسرطان البروستاتا، فناقِش الخيارات المتاحة مع طبيبك. وتشمل أنواع العلاج الهرموني لسرطان البروستاتا ما يلي:
- أدوية تمنع الخصيتين من إنتاج التستوستيرون. تمنع بعض الأدوية الخلايا من تلقي الإشارات التي توجِّهها إلى إنتاج التستوستيرون. ويُطلَق على هذه الأدوية ناهضات ومناهضات الهرمون المُطلِق لهرمون اللَّوْتَنة (LHRH). من الأسماء الأخرى لهذه الأدوية ناهضات ومناهضات الهرمون المُطلِق لموجِّهة الغدد التناسلية.
- أدوية تمنع التستوستيرون من التفاعل مع الخلايا السرطانية. هذه الأدوية، التي تُعرَف بمضادات الأندروجينات، تُستخدَم عادةً مع ناهضات الهرمون المُطلِق لهرمون اللَّوْتَنة. ويرجع ذلك إلى أن هذه الناهضات يمكن أن تسبب ارتفاعًا وجيزًا في مستويات هرمون التستوستيرون، ثم أن تنخفض مرة أخرى.
- جراحة لإزالة الخصيتين، يُطلَق عليها استئصال الخصيتين. تسهم الجراحة التي تُجرى لاستئصال الخصيتين في خفض مستويات التستوستيرون في الجسم سريعًا. ومن خلال أحد أنواع هذا الإجراء الطبي، تُستأصل الخلايا التي تنتج التستوستيرون فقط، ولا تُستأصل الخصيتان. ولا يمكن الرجوع إلى الوضع السابق لجراحة استئصال الخصيتين بعد إجرائها.
ما يمكنك توقعه
ناهضات ومناهضات الهرمون المطلِق لهرمون اللَّوتَنة
تمنع ناهضات ومناهضات الهرمون المُطلِق لهرمون اللَّوْتَنة (LHRH) الخصيتين من إنتاج التستوستيرون.
تُعطى معظم هذه الأدوية عن طريق حقنها تحت الجلد أو في عضلة. وتُعطى كل شهر أو ثلاثة أو ستة أشهر. أو يمكن وضعها تحت الجلد كغريسة. وتُطلِق الغريسة الأدوية ببطء بمرور الوقت.
تشمل ناهضات الهرمون المُطلِق لهرمون اللَّوْتَنة ما يلي:
- ليوبروليد (Eligard و Lupron Depot وغيرهما)
- غوسيريلين (Zoladex)
- تريبتوريلين (Trelstar)
تشمل مناهضات الهرمون المُطلِق لهرمون اللَّوْتَنة ما يلي:
- ديغاريليكس (Firmagon)
- ريلوجوليكس (Orgovyx)
قد تزيد مستويات هرمون التستوستيرون لفترة وجيزة، ويُسمى ذلك بالوهيج، لبضعة أسابيع بعد تلقي ناهض الهرمون المُطلِق لهرمون اللَّوْتَنة. ولا تسبب مناهضات الهرمون المُطلِق لهرمون اللَّوْتَنة وهيج التستوستيرون.
منع حدوث الوهيج هو أمر مهم لمن يشعرون بالألم أو بأي أعراض أخرى للسرطان. فقد تسبب زيادة مستويات التستوستيرون تفاقم الأعراض. يمكن أن يساعد تناوُل الأدوية المضادة للأندروجينات قبل أو مع تناوُل ناهضات الهرمون المُطلِق لهرمون اللَّوْتَنة في تقليل احتمال حدوث الوهيج.
مضادات الأندروجين
تمنع الأدوية المضادة الأندروجينات التستوستيرون من التفاعل مع الخلايا السرطانية. يتناول المريض هذه الأدوية غالبًا مع ناهضات الهرمون المطلق لهرمون اللَّوْتَنة أو قبل تناول تلك الناهضات.
تشمل الأدوية المضادة للأندروجينات ما يلي:
- بيكالوتاميد (Casodex)
- فلوتامايد
- نيليوتاميد (Nilandron)
- أباليوتاميد (Erleada)
- داروليوتاميد (Nubeqa)
- إينزاليوتاميد (Xtandi)
استئصال الخصية
نادرًا ما يُستخدَم هذا العلاج لاستئصال الخصيتين. بعد تخدير منطقة الأُربية، يُحدِث الجرَّاح شقًا في الأُربية ويستأصل الخصية من الفتحة، ثم يكرر نفس العملية لاستئصال الخصية الأخرى.
تنطوي الجراحة عمومًا على احتمال التعرض للألم وحدوث نزيف والإصابة بعدوى. ويستطيع معظم الأشخاص العودة إلى المنزل بعد هذه العملية. ولا تستدعي الحالة عادةً الإقامة في المستشفى.
النتائج
إذا كنت تتلقى علاجًا هرمونيًا لسرطان البروستاتا، فعليك زيارة الطبيب بانتظام لمتابعة حالتك. سيطرح عليك الطبيب أسئلة عن الآثار الجانبية التي تشعر بها. تجدر الإشارة إلى أنه يمكن السيطرة على العديد من الآثار الجانبية.
وقد يطلب منك الطبيب إجراء اختبارات لتقييم حالتك الصحية والبحث عن مؤشرات على احتمال الإصابة بالسرطان مجددًا أو تفاقمه. يمكن أن تُظهر نتائج هذه الاختبارات مدى استجابتك للعلاج الهرموني. ويمكن تعديل العلاج حسب الحاجة.
Hormone therapy resistance
Over time, most prostate cancers eventually become resistant to ADT. This means the hormone therapy stops working. The cancer continues to grow even when testosterone levels are very low. You might hear this type of cancer called castration resistant, hormone resistant or androgen resistant. You also might hear it called hormone-refractory prostate cancer (HRPC).
It's difficult to predict how long until a prostate cancer becomes resistant to ADT. About half of those treated with ADT become resistant within 2 to 3 years. And about half become resistant after more than 2 to 3 years.
Your healthcare professional likely will order regular testing to check your health and to see if the cancer is coming back or getting worse. These tests can show your response to ADT.
If your cancer appears to become resistant, you generally continue taking hormone therapy. This is to keep testosterone levels low. If testosterone levels go up, it could make the cancer grow or get worse.
A healthcare professional may suggest a different hormone therapy. Or you might also be given another type of medicine, depending on your situation. Other medicines could include:
- Chemotherapy.
- A type of medicine that contains radioactive material, called a radiopharmaceutical.
- A type of medicine called a poly(ADP-ribose) polymerase (PARP) inhibitor. This could be an option if you have certain gene changes.
- A type of medicine that targets your immune system, called immunotherapy. This might be an option if you have a certain type of tumor.
Survival rates
How long someone lives with prostate cancer after starting hormone therapy can be different for each person. It depends on things like the stage of the cancer and how far it has spread. Your healthcare professional may be able to give you more exact information based on your condition.