نظرة عامة
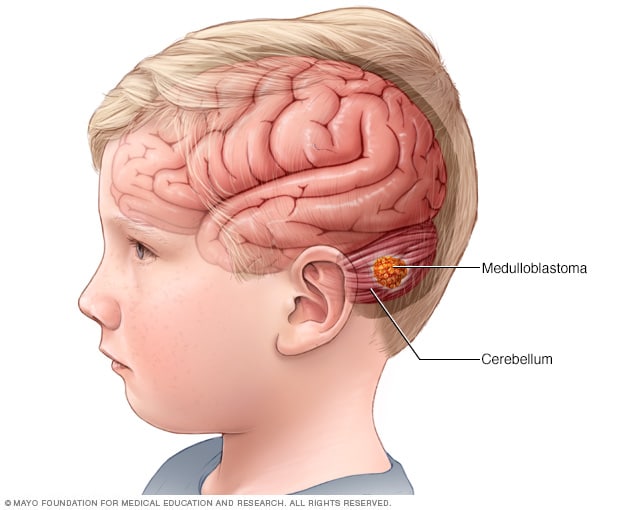
الورم الأرومي النخاعي ورم دماغي سرطاني يبدأ في الجزء السفلي الخلفي من الدماغ. يُسمى هذا الجزء من الدماغ المخيخ. ويؤدي دورًا في تناسق العضلات والتوازن والحركة.
يبدأ الورم الأرومي النخاعي في صورة نمو للخلايا يُسمى ورمًا. وتنمو الخلايا سريعًا ويمكن أن تصل إلى أجزاء أخرى من الدماغ. غالبًا تنتشر خلايا الورم الأرومي النخاعي في السائل المحيط بالدماغ والحبل النخاعي ويحميهما. ويُسمى ذلك السائل بالسائل الدماغي النخاعي. ولا تنتشر الأورام الأرومية النخاعية عادةً في أجزاء أخرى من الجسم.
يمكن أن يحدث الورم الأرومي النخاعي في أي سن، لكنه غالبًا يصيب الأطفال الصغار. وعلى الرغم من أن الورم الأرومي النخاعي نادر الحدوث، فإنه أكثر أورام الدماغ السرطانية شيوعًا لدى الأطفال. ويكثر شيوع الورم الأرومي النخاعي في العائلات التي لديها سيرة مرضية من الحالات التي تزيد من احتمال الإصابة بالسرطان. وتشمل هذه المتلازمات متلازمة غورلين أو متلازمة تركو.
المنتجات والخدمات
Types
The type of medulloblastoma is based on how the tumor cells look under a microscope and on lab tests that look at changes in the tumor's genes. The type of medulloblastoma helps guide treatment and can affect survival.
All medulloblastomas are considered grade 4 tumors. The subtypes below describe the tumor's molecular features, not its grade.
Molecular types
Most medulloblastomas can be grouped into four main types based on changes in their genes. These tumor types include:
- WNT-activated (wingless/integrated). WNT is the name of a cell signaling pathway involved in brain development. WNT-activated tumors are one of the less common medulloblastoma types. They often respond very well to treatment and are linked to the best survival rates. They are most often seen in older children and teens.
- SHH-activated (sonic hedgehog). Sonic hedgehog is the name of a cell growth signaling pathway involved in brain development. SHH medulloblastoma can occur in infants, children and adults. Survival varies depending on other tumor features and gene changes. Some SHH tumors, known as SHH-activated TP53-wildtype, behave less aggressively. Other SHH tumors, called SHH-activated TP53-mutant, may be harder to treat.
- Group 3. Group 3 medulloblastoma is more common in young children. These tumors are non-SHH and non-WNT molecular types. It tends to grow and spread more quickly than other types. It may be harder to treat and is often linked to lower survival rates compared with WNT tumors.
- Group 4. Group 4 medulloblastoma is the most common type. These tumors are non-SHH and non-WNT molecular types. It can occur in children and adults. Its behavior varies. Some tumors respond well to treatment, while others may spread at diagnosis.
The numbering starts at 3 and 4 because the first two groups were named WNT-activated and SHH-activated based on specific gene patterns.
Cell appearance types
Medulloblastoma also can be described based on how the cells look under a microscope although genetic and molecular features are increasingly used for diagnosis and understanding outcomes. These include:
- Classic.
- Desmoplastic or nodular.
- Large cell or anaplastic.
These features also help healthcare professionals understand how the tumor may behave.
How is medulloblastoma different from other brain tumors?
Medulloblastoma is different from many other types of brain tumors. These tumors differ in where they start, who they affect and how they are treated.
Here's how they compare:
- Medulloblastoma versus glioma. Medulloblastoma is not a glioma. Gliomas form from support cells in the brain called glial cells. Medulloblastoma forms from developing nerve cells in the cerebellum.
- Medulloblastoma versus glioblastoma. Glioblastoma is an aggressive brain tumor that usually affects adults and starts in the upper parts of the brain. Medulloblastoma is more common in children and often responds better to treatment.
- Medulloblastoma versus ependymoma. Ependymomas begin in cells that line the fluid-filled spaces of the brain and spinal cord. Medulloblastoma tends to grow in the cerebellum and is more likely to spread through cerebrospinal fluid.
الأعراض
الورم الأرومي النخاعي
الورم الأرومي النخاعي
يُعد الورم الأرومي النخاعي نوعًا من سرطان الدماغ، والذي يبدأ في جزء بالدماغ معروف باسم المخيخ. ويُعد الورم الأرومي النخاعي أكثر أورام الدماغ السرطانية شيوعًا لدى الأطفال.
تحدث أعراض الورم الأرومي النخاعي عندما ينمو السرطان أو يؤدي إلى زيادة الضغط داخل الدماغ. وقد تشمل مؤشرات الورم الأرومي النخاعي وأعراضه:
- الدوخة.
- ازدواج الرؤية.
- الصداع.
- الغثيان.
- ضَعف التناسق.
- التعب.
- عدم اتزان المشية.
- القيء.
Symptoms in young children and infants
In young children, symptoms may develop over several weeks. Children may have trouble walking, seem clumsy or lose balance. Infants may have an increase in head size, unusual sleepiness or feeding difficulties.
Symptoms in children and adults
Symptoms of medulloblastoma are generally similar in adults and children because the tumor usually starts in the same part of the brain. Both may have headaches, balance difficulties and nausea.
Can you feel a medulloblastoma tumor?
Medulloblastoma grows deep inside the brain. It does not usually cause a lump or bump that you can feel on the outside of the head.
الحالات التي تستلزم زيارة الطبيب
حدِّد موعدًا طبيًا مع الطبيب أو أي اختصاصي رعاية صحية آخر إذا ظهرت عليك أي أعراض تثير قلقك.
الأسباب
ليس من الواضح ما يسبب الورم الأرومي النخاعي. يبدأ هذا السرطان بنمو الخلايا في الدماغ.
تحدث الإصابة بالورم الأرومي النخاعي عندما تطرأ تغيرات على الحمض النووي للخلايا الموجودة في الدماغ. يحمل الحمض النووي للخلية التعليمات التي توجِّه الخلية لأداء وظيفتها. كما يعطي الحمض النووي في الخلايا السليمة أوامر بالنمو والتكاثر بمعدل ثابت. وتوجِّه التعليمات الخلايا إلى أن تموت في وقت محدد. تعطي تغيرات الحمض النووي تعليمات مختلفة في الخلايا السرطانية. توجه هذه التغييرات الخلايا السرطانية إلى النمو والتكاثر بسرعة. ويمكن أن تستمر الخلايا السرطانية في البقاء في حين قد تموت الخلايا السليمة. ويؤدي ذلك إلى وجود عدد كبير جدًا من الخلايا.
تشكل الخلايا السرطانية كتلة تُسمى ورمًا يمكن أن تنمو لتضغط على الهياكل المجاورة. وقد تغزو الخلايا السرطانية أنسجة الجسم السليمة وتدمرها. ويمكنها أيضًا الانتشار إلى مناطق أخرى.
عوامل الخطورة
تشمل العوامل التي قد تزيد من خطورة الإصابة بالورم الأرومي النخاعي ما يأتي:
- السن الصغيرة. يمكن أن يحدث الورم الأرومي النخاعي في أي مرحلة عمرية. ويحدُث هذا السرطان في أغلب الأحيان عند الأطفال.
- المتلازمات الموروثة. ويكثر شيوع الورم الأرومي النخاعي في العائلات التي لديها سيرة مرضية من الحالات التي تزيد من احتمال الإصابة بالسرطان. وتشمل هذه الحالات فقر الدم فانكوني ومتلازمة غورلين ومتلازمة لي فراوميني ومتلازمة روبينستاين-تيبي ومتلازمة تركو.