Aug. 27, 2019
Male stress incontinence can be devastating, and treatment can significantly improve patient well-being and quality of life.
"For severe stress incontinence, the gold standard treatment is implantation of an artificial urinary sphincter. However, the most important factor compromising outcomes remains device infection, with a prevalence of 3% to 8% in the literature ― 1.8% in Mayo Clinic's experience since 1983," says Daniel S. Elliott, M.D., with Urology at Mayo Clinic's campus in Rochester, Minnesota. "This complication requires device removal. Therefore, development of strategies to reduce the incidence of infection and erosion is of the utmost importance."
The no-touch technique for implantation of inflatable penile prosthesis, developed by Jean-Francois Eid, M.D., is based on the concept that device infection is due to direct inoculation with local skin flora at the time of surgery. This concept is well established in other fields with device implantation, such as orthopedics, neurosurgery and plastic surgery. The no-touch technique was published in the Journal of Sexual Medicine in 2011.
"In inflatable penile prosthesis surgery, this approach has led to an infection rate of less than 0.5% in Dr. Eid's experience," says Dr. Elliott. "However, there is a relative paucity of data applying this concept to artificial urinary sphincter placement. Starting in 2014, Mayo Clinic implemented a minimal-touch protocol for artificial urinary sphincter placement to minimize perineal and abdominal skin exposure. This protocol has decreased the rate of device infection."
The minimal-touch protocol includes standard infection preventive measures, such as the administration of the standardized perioperative antibiotics vancomycin and gentamicin, wide skin prep with chlorhexidine-based solution, and standard surgical draping. After that, the following steps are applied:
- An Ioban incise drape is placed over the anterior abdominal wall to cover exposed skin to the level of the penopubic junction.
- An additional Ioban incise drape is then placed along the posteromedial thighs and across the perineum, just under the junction of the posterior scrotum and perineum.
- The penis and scrotum are left exposed and a 12-French urethral catheter is placed. Then the scrotum is covered with a surgical lap pad and retracted away from the perineal incision.
- Copious wound irrigation with an antibiotic solution of gentamicin, neomycin and polymyxin is performed prior to device placement. Outer gloves also are changed at this point.
- During the placement of the device into the perineal wound, care is taken to avoid any contact with skin that may have been exposed under the Ioban incise drape, and an antibiotic-soaked lap pad is placed over the device prior to the abdominal portion of the procedure. This lap pad is then placed in a sterile plastic bag and secured to the Ioban incise drape. Outer gloves are once again changed and an abdominal incision is made.
- Prior to the placement of the pressure-regulating balloon, the abdominal wound is also irrigated copiously.
- After a Hegar dilator is used to develop a plane between the abdominal wall incision and ipsilateral hemiscrotum, the pump is placed via the abdominal incision.
- The cuff tubing is then carefully delivered to the abdominal incision and cut to length, and all components are attached via Quick Connects.
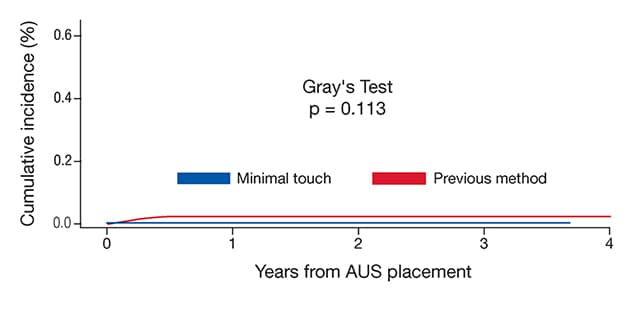
Gray's test evaluation of incidence
Gray's test evaluation of incidence
For this study, none of the 433 patients who underwent minimal-touch technique experienced device infection. Of the 1,253 patients who underwent standard artificial urinary sphincter placement, 28 had device infection.
Of the 2,535 patients who underwent artificial urinary sphincter placement and met inclusion criteria for this unpublished study, none of the 433 patients who underwent minimal-touch technique experienced device infection. Of the 1,253 patients who underwent standard artificial urinary sphincter placement, 28 had device infection.
"Statistical analysis is ongoing, but the lack of any infection in the minimal-touch cohort is certainly encouraging and merits further study," says Dr. Elliott. "Furthermore, the majority of infections occurred early, supporting the hypothesis that the majority of infections are due to contamination with skin flora at the time of device placement."
For more information
Eid JF. Surgical techniques: No-touch technique. Journal of Sexual Medicine. 2011;8:5.