March 19, 2021
Elizabeth Ann L. Enninga, Ph.D., an immunologist at Mayo Clinic's campus in Rochester, Minnesota, is studying villitis of unknown etiology (VUE), a placental condition that is inflammatory, not infectious like cytomegalovirus, Toxoplasma gondii or HIV. Findings from the study were published in The Journal of Immunology in April 2020.
In this research, Dr. Enninga and team performed immunosequencing for precise T cell identification from placentas in the following categories: normal; infectious, especially cytomegalovirus; and VUE. The team also investigated triggers for VUE activity and observed distinct differences between VUE and infectious villitis. They discerned the following:
- VUE is maternally driven — the mother's immune system targets the baby (placenta), whereas in infectious villitis the baby's immune system is fighting off the infection.
- VUE represents a T cell immune response unique to the mother and baby, versus infectious villitis, which shows common T cells in each placenta fighting the pathogen.
الخلايا التائية للأم في مشيمة الجنين أثناء تشخيص التهاب الزغابات مجهول السبب
الخلايا التائية للأم في مشيمة الجنين أثناء تشخيص التهاب الزغابات مجهول السبب
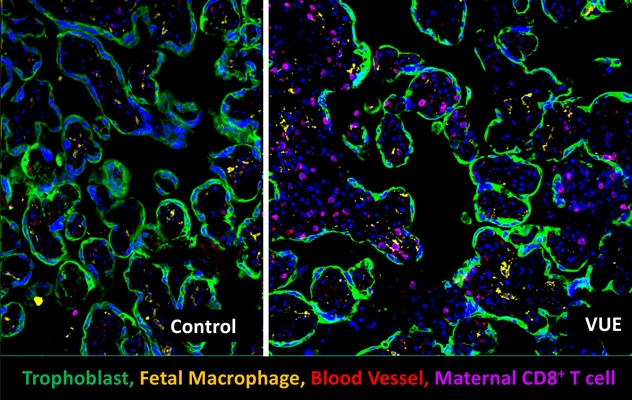
تظهر الخلايا التائية للأم في مشيمة الجنين أثناء تشخيص التهاب الزغابات مجهول السبب، ولكن ليس في المشيمة الطبيعية (الخاصة بالمراقبة).
"VUE really is its own condition, not an undiagnosed infection," says Dr. Enninga. "VUE is unlike and more complex than an infection, in that the fetal allograft is unique to each pregnancy."
The recognition of VUE as a distinct condition is significant because it identifies the need for specific VUE diagnosis and treatment methods, each of which are challenging for this condition currently.
"With an infection, it's easier to diagnose during pregnancy, as mom and baby will have symptoms," says Dr. Enninga. "We're not good at recognizing inflammation if there are no symptoms, and therefore we don't have great tools to prevent or treat noninfectious inflammation."
It's also crucial to identify VUE when it occurs in pregnancy, as it presents significant risk for the fetus and the mother's subsequent pregnancies. When identified, physicians can follow the mother and counsel her if she plans to have more children.
"If we are not addressing this maternal immune response that is targeted toward the baby, we're just rolling the dice on what's going to happen next," says Dr. Enninga. "You develop these CD8+ T cells, and they can come back stronger in another pregnancy."
VUE background and need for translational collaboration
VUE is the infiltration of maternal cytotoxic T cells, which attack the placenta's vasculature. At times, this condition has no apparent effect, and at other times it is associated with growth restriction, miscarriage and demise, or preterm birth. An expectant mother's immune system normally tolerates the genetically unique fetus to safely carry the baby, yet in VUE this tolerance appears to be lost.
The general concept of VUE — though argued to be an undiagnosed infection — has been around since 1975. True to its name, the scientific community doesn't know what triggers it, says Dr. Enninga. It's currently diagnosed postnatally in pathological review of the placenta. She mentions, however, that the idea of VUE as a distinct entity with clinical relevance is new to many physicians.
VUE's incidence is difficult to pinpoint, says Dr. Enninga, indicating it may occur in 6% to 33% of pregnancies, according to an article in the journal APMIS. She hopes to better quantify the incidence, along with subsequent pregnancy recurrence risk, currently described in the same article as 10% to 30%. The challenge for pinpointing these figures is that placental pathology is not routinely performed at all institutions.
Dr. Enninga indicates that one aspect she appreciates about her work at Mayo Clinic is its strong placental pathology group, which is rare among academic medical centers. This group works closely with her lab to understand complex pregnancy cases and provide the ability to look back on complicated cases to better counsel patients.
Dr. Enninga states her goal is to bring obstetricians and pathologists together to work in tandem on VUE and its screening. "My focus is how I can make findings in the lab useful for physicians caring for patients," she says.
VUE detection and therapy research
Currently, VUE can only be detected postnatally. However, Dr. Enninga is working to identify an effective VUE screening method using blood or ultrasound tools or both. She indicates that blood testing is conducted during pregnancy currently, which can measure important variables such as Rh factor compatibility, blood glucose and fetal aneuploidy. Screening for VUE, however, may involve blood testing throughout pregnancy to see if the mother's body is mounting an immune response against the baby.
Dr. Enninga and team are collaborating on microvessel ultrasound research with Shigao Chen, Ph.D., a Mayo Clinic diagnostic radiology investigator, and seeking to map blood vessels to discover if differences exist in cases of VUE. Predicting Placental Pathologies by Ultrasound Imaging, an NIH-funded clinical trial, is an observational cohort enrolling women diagnosed with intrauterine growth restriction (IUGR) to discern whether VUE-related differences are visible by ultrasound, as VUE is present in many infants diagnosed with IUGR. As VUE often occurs later in pregnancy, Dr. Enninga indicates the investigators' ultimate hope is to monitor for VUE in the third trimester and negate the risks associated with this diagnosis.
"When the baby is still in the womb, we can actually do something," says Dr. Enninga. "By the time VUE is diagnosed by pathology, it's too late."
Early diagnosis of VUE and the ability to follow its development are key to future therapeutic moderation, Dr. Enninga says. "If we can routinely identify it, we can stop it. Then we need to find a therapy to pacify mom's immune system, telling it, 'Hey, calm down — leave that baby alone.'"
Clinical relevance for obstetricians and family medicine
Though Dr. Enninga admits her findings on VUE are not fully clinically relevant yet, Regan N. Theiler, M.D., Ph.D., chair of Obstetrics at Mayo Clinic's campus in Rochester, Minnesota, believes this is an important step in the right direction.
"Traditionally, placental pathology findings have been helpful in explaining problems with the previous pregnancy, but not helpful in prediction or prevention of complications of future pregnancies," Dr. Theiler says. "Dr. Enninga's work aims to change the state of the science on this."
Dr. Enninga encourages those following pregnant mothers to pay careful attention to pathology reports and work closely with a pathologist if concerns arise. As the clinical trial chaired by Dr. Enninga is accruing currently, physicians also may refer patients to determine if they meet eligibility criteria.
For more information
Enninga EAL, et al. Maternal T cells in the human placental villi support an allograft response during noninfectious villitis. The Journal of Immunology. 2020;204:2931.
Chen A, et al. Placental pathologic lesions with a significant recurrence risk — What not to miss! APMIS. 2018;126:589.
Mayo Clinic. Predicting Placental Pathologies by Ultrasound Imaging. ClinicalTrials.gov.