Dec. 31, 2020
Mayo Clinic has described a new clinical sign that is highly specific for the diagnosis of multiple sclerosis (MS). In a technician-blinded study, Mayo researchers found that McArdle sign — a clinical phenomenon in which neck flexion induces rapid, reversible weakness — is also moderately sensitive for a diagnosis of MS when compared with other myelopathy conditions that mimic MS.
"This is a unique sign that to our knowledge has not been used in clinical practice elsewhere," says Brian G. Weinshenker, M.D., a neurologist at Mayo Clinic in Rochester, Minnesota. "The sign is easily demonstrated at the bedside, so this finding can be immediately translated into practice."
MS is commonly misdiagnosed, due to the lack of clinical signs and MRI findings specific to the disease. Dr. Weinshenker notes that approximately 20% of patients referred to his practice with a diagnosis of MS don't have the disease; some of these patients have taken MS disease-modifying therapies for years. Similar observations have been made at other large medical centers. "McArdle sign is another arrow in our quiver — a specific finding that indicates MS and not another myelopathy," Dr. Weinshenker says.
Dr. Weinshenker first observed the phenomenon in the 1980s, in a patient with advanced MS. "He would arch his neck every time he took a step. When we asked him to put his chin down, he couldn't walk," Dr. Weinshenker says.
Around the same time, Dr. Weinshenker read a case report in the Journal of Neurology, Neurosurgery, and Psychiatry that described the phenomenon in a patient in England. The authors of that 1987 report were students of the neurologist M.J. McArdle, and named the phenomenon after him.
Los músculos extensores de los dedos proporcionan un medio conveniente para evaluar la esclerosis múltiple
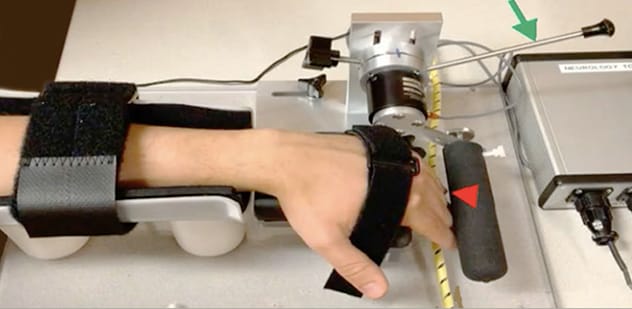
Los músculos extensores de los dedos proporcionan un medio conveniente para evaluar la esclerosis múltiple
El médico intenta superar la resistencia del paciente a la extensión de los dedos, comprobando si hay una disminución de la fuerza cuando la prueba se realiza con el cuello en flexión en comparación con el cuello en extensión.
No further reports on McArdle sign were published. But over the next several decades, Dr. Weinshenker evaluated the sign in his clinical practice and taught it to Mayo Clinic residents. Finger extensor muscles, which are among the first muscles to weaken in people with MS, provide a convenient means of testing: The physician attempts to overcome a patient's resistance of finger extension, checking for a decrease in strength when the test is performed with neck flexion compared with neck extension.
"I found lots of patients who demonstrated this phenomenon to varying degrees," Dr. Weinshenker says. "It was often the only clinical sign of MS. Patients with symptoms of the disease might have a completely normal clinical exam, with normal reflexes and strength — but they lost strength with neck flexion. The patients are usually shocked when I find this sign."
Quantitative evaluation
Mayo Clinic researchers have now quantitated McArdle sign. Their pilot study, described in the August 2019 issue of Mayo Clinic Proceedings, included 50 patients with MS, 25 patients with other causes of myelopathy, five patients with finger weakness due to peripheral nerve lesions and 25 healthy participants.
For each participant, a technician attempted to overcome maximal resistance of finger extension in successive trials of neck extension and flexion. Any clinically perceived decline in strength with neck flexion was rated.
Datos sin procesar de pruebas isoinerciales de tres participantes representativos del estudio
McArdle sign was then quantitated in each participant, using a torque measurement device developed at Mayo Clinic for the study by Lawrence Berglund, a biomedical engineer. The device allowed for both isometric and isoinertial testing. The peak strengths in neck flexion and extension were recorded for each study participant.
"We found that a 10% or greater decrease in strength during neck flexion was 100% specific and about 70% sensitive for MS compared to other myelopathies," Dr. Weinshenker says. "A decrease in strength of 5% to 10% is a gray area that is suggestive of MS but not entirely specific."
Both the average isometric and isoinertial torque reductions correlated with the blinded clinical evaluation of McArdle sign. "The clinical detection of a flexion-induced decrease in strength is quite reliable when compared with the decrease in strength measured by our device, especially when the decline is moderate or marked," Dr. Weinshenker says.
The pathophysiology of McArdle sign is uncertain. But the Mayo Clinic researchers speculate it might be due to a nerve conduction block induced by the mechanical stretching of the spinal cord with neck flexion. "We're undertaking studies with motor evoked potentials to address this possibility," Dr. Weinshenker says.
If that possibility is borne out, McArdle sign potentially might help identify patients who would benefit from treatment with conduction-enhancing medications such as dalfampridine. Dr. Weinshenker notes that only about one-third of patients with MS respond well to dalfampridine; in his experience, people who exhibit a strong McArdle sign are often the best responders. The phenomenon might indicate that despite demyelination, these patients have sufficient viable axons to overcome conduction block with medication. "But the pathophysiology of this phenomenon must be further addressed," Dr. Weinshenker says.
The immediate value of McArdle sign is its straightforward application to patient care. "When you observe a clinical sign in very extreme form, you can be more confident in a diagnosis of MS; it is more valuable when present than when it is absent," Dr. Weinshenker says. "We hope that McArdle sign's clinical value for diagnosis will spread beyond Mayo Clinic."
For more information
O'Neill JH, et al. McArdle's sign in multiple sclerosis. Journal of Neurology, Neurosurgery, and Psychiatry. 1987;50:1691.
Savoldi F, et al. McArdle sign: A specific sign of multiple sclerosis. Mayo Clinic Proceedings. 2019;94:1427.