May 22, 2014
休息和排便时的耻骨直肠肌
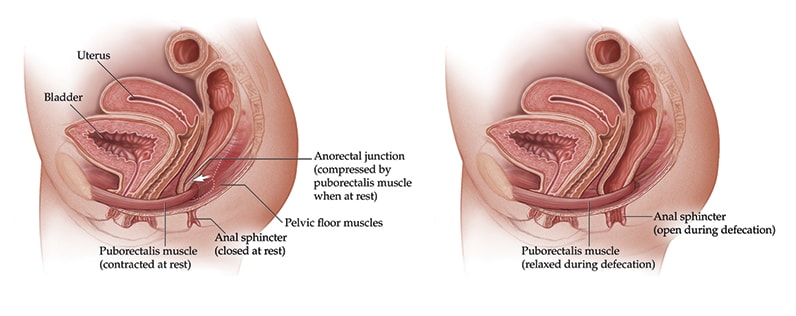
休息和排便时的耻骨直肠肌
多达 50% 的慢性便秘患者患有盆底功能障碍 (PFD),这会导致盆底和腹肌在排便期间无法正常放松和协调。
As many as 50 percent of people with chronic constipation have pelvic floor dysfunction (PFD) — impaired relaxation and coordination of pelvic floor and abdominal muscles during evacuation. Straining, hard or thin stools, and a feeling of incomplete elimination are common signs and symptoms. But because slow transit constipation and functional constipation can overlap with PFD, some patients may also present with other signs and symptoms, such as a long time between bowel movements and abdominal pain.
When mechanical, anatomic, and disease- and diet-related causes of constipation have been ruled out, clinical suspicion should be raised to the possibility that PFD is causing or contributing to constipation. A focused history and digital examination are key components in diagnosing PFD. The diagnosis can be confirmed by anorectal manometry with balloon expulsion and, in some cases, traditional proctography or dynamic magnetic resonance imaging defecography to visualize pathologic pelvic floor motion, sphincter anatomy and greater detail of surrounding structures.
To help patients restore normal bowel function, Mayo Clinic staff use a multidisciplinary approach that can include:
- Constipation education classes led by a dietitian and a nurse educator
- Intensive pelvic floor retraining exercises
- Biofeedback training
- Behavior modification
Patients may meet individually with a dedicated nurse educator who provides a focused session on bowel management techniques. Central to the process is a daily regimen that combines an evening dose of fiber supplement with a morning routine of mild physical activity; a hot, preferably caffeinated beverage; and, possibly, a fiber cereal followed by another cup of a hot beverage — all within 45 minutes of waking. This routine augments early morning high-amplitude peristaltic contractions by incorporating multiple colon stimulators.
The regimen, useful for many types of constipation, is fine-tuned for PFD. Some patients do not need fiber; others may need to supplement with occasional laxatives. The program can change over time as patients make advancements.
Biofeedback to retrain pelvic floor muscles
Once patients with pelvic floor constipation have these basic tools, they can begin retraining the pelvic floor muscles with biofeedback. Based on the principle of operant conditioning, biofeedback provides auditory and visual feedback to help retrain the pelvic floor and relax the anal sphincter. Biofeedback training is the treatment of choice for medically refractory pelvic floor constipation, with some studies showing improvement in more than 70 percent of patients. Patients also learn to identify internal sensations associated with relaxation and long-term skills and exercises for use at home.
Although many centers are familiar with retraining techniques to improve pelvic floor dysfunction, few have the multidisciplinary expertise to teach patients with constipation how to appropriately coordinate abdominal and pelvic floor muscles during defecation, and how to use bowel management techniques, along with behavior modification, to relieve symptoms. Because pelvic floor dysfunction can be associated with psychological, sexual or physical abuse and other life stressors, psychological counseling is often included in the evaluation process.
Mayo Clinic's experience using a multidisciplinary approach to treating PFD has yielded positive patient outcomes. In some patients, the improvement is minor, and in others, it can be life-changing.