May 31, 2025
The American Academy of Pediatrics recommends that children age 5 and older engage in at least 60 minutes of physical activity a day, which should include a mix of moderate to vigorous intensity aerobic exercise and bone-strengthening activities at least three days a week. Children are encouraged to be active for their health, but with activity and sports participation inevitably comes injuries. Some injuries are minor, while others can be more serious, such as fractures and ligament ruptures. By the age of 16, 40% of boys and 25% of girls will have broken a bone. Hand and wrist fractures in children are very common, and the risk is even higher for those who participate in sports. While the most common of these injuries is a distal radius fracture, an increasing number of children are experiencing scaphoid fractures.
Scaphoid fractures are less frequent in children under 10 because the scaphoid bone is still developing and is largely cartilaginous. The ossification of the scaphoid starts around ages 4 to 6 and continues until ages 13 to 15, where pediatric scaphoid fractures become more common as the bone becomes more fully ossified.
"Children with scaphoid fractures are typically older than the age of 10, and they are often in high-contact activities like hockey, basketball and football," says Nicholas A. Pulos, M.D., a pediatric orthopedic surgeon at Mayo Clinic in Rochester, Minnesota.
Children with suspected scaphoid fractures may experience pain and tenderness in the anatomical snuff-box, limited wrist range of motion and bruising.
"The cartilaginous nature of the scaphoid in younger children can make diagnosing fractures more challenging, as they may not be as easily visible on initial X-rays," says Dr. Pulos.
Delays in treatment can lead to more complicated surgical needs, arthritis and carpal instabilities.
"The blood supply to the scaphoid is fairly tenuous, so not all fractures heal on their own," says Dr. Pulos. "There is a high nonunion risk with this type of injury, so it's important to get the right care the first time."
Depending on the severity of the injury, immobilization with a cast and pausing contact sports can be enough to allow healing to take place. In other cases, a child might need surgery.
"Currently, the standard of care for kids who have a suspected scaphoid fracture but have negative X-rays is to follow up with either another X-ray or advanced imaging," says Dr. Pulos. "We'd recommend immobilization and repeat radiographs after about 10 days. Fractures are more clearly seen at that time because of the body's own healing process."
If a scaphoid fracture is not diagnosed right away or if complications occur, there is a higher risk of nonunion that can affect a child's ability to do everyday activities.
"There are two things that scaphoids need to properly heal," says Dr. Pulos. "They need good stability, and they also need good biology. Sometimes it can be treated without surgery, but the nuance between the two can be pretty fine."
Although most scaphoid fractures in pediatric patients heal with proper treatment, nonunion, proximal pole avascular necrosis and carpal malalignment can occur.
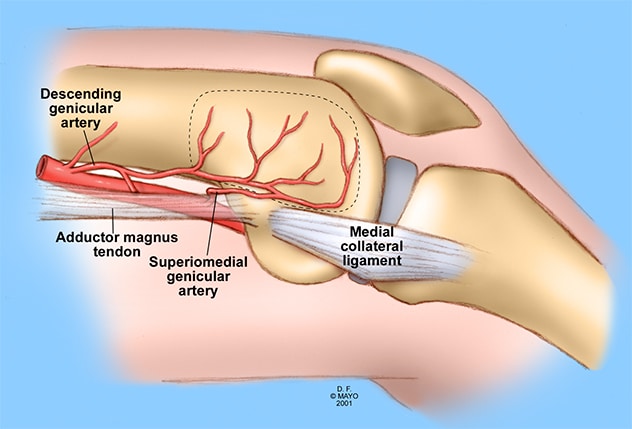 Anatomía vascular del colgajo del cóndilo femoral medial
Anatomía vascular del colgajo del cóndilo femoral medial
Sitio del injerto óseo corticoperióstico en el fémur distal y anatomía vascular circundante. Representación esquemática de las estructuras anatómicas del fémur distal medial con delineado del injerto.
 Fractura de escafoides
Fractura de escafoides
Reparación de injerto óseo en forma de cuña. Cirugía de muñeca, abordaje dorsal. Revascularización con injerto de vaso del antebrazo. Vista palmar.
Vascularized bone grafts have shown promising results in adult scaphoids with compromised vascularity. Recently, Dr. Pulos and a team of researchers studied whether this approach would have similar outcomes in adolescents.
In the October 2024 issue of Journal of Hand Surgery, Mayo Clinic researchers found that adolescent patients treated for scaphoid nonunion with a vascularized bone graft from either the medial femoral condyle or dorsal distal radius had an 85% union incidence, improved carpal alignment and a low incidence of complications.
All scaphoid nonunions have some degree of bone loss that almost always requires adding a bone graft. Sometimes, part of the scaphoid loses its blood supply, which requires bone graft and blood supply. Sometimes the scaphoid 'collapses' — for example, folding over at the nonunion site or break — and requires bone graft that is structural.
"Sometimes these scaphoid nonunions have both decreased blood supply and collapse," says Dr. Pulos. "These need a specialized bone graft that is both vascular and structural. Matching the type of bone graft to the nonunion is key. At Mayo Clinic Children's, we have access to the breadth and depth of resources needed to complete the necessary surgeries based on the child's individual needs."
For patients needing this type of surgery, Mayo Clinic specialists employ a two-team approach. One surgeon approaches the scaphoid for the bone reconstruction, and another surgeon can harvest the bone flap at the same time.
"Doing both of these procedures simultaneously helps us each focus on our own part of the procedure, while also giving the opportunity to put our heads together to problem-solve in real time," says Dr. Pulos.
Mayo Clinic is also one of the only centers in the United States using photon-counting detector CT scans, which is an advantage in the treatment of adolescents with nonunion scaphoid fractures.
"This allows us to closely assess the bony architecture — structures that were simply too small to be resolved with previous detector technologies," says Dr. Pulos. "Also, I typically need a patient to have one CT prior to surgery and then another one afterwards to assess how they're healing. Another advantage of the photon-counting CT is that it can achieve the same image quality of a conventional CT scan with about a 50% reduction in radiation."
With increasing opportunities for children to participate in sports and high-contact activities year-round, injuries are common. But quick action combined with an enhanced approach to treatment is key.
"With the right care at the right time, our goal is that these kids are getting back to the sports and activities they enjoy as safely and as quickly as possible," says Dr. Pulos.
For more information
Israel JS, et al. The role of vascularized bone grafting for scaphoid nonunions in adolescents. Journal of Hand Surgery (European Volume). 2024;49:1157.
Refer a patient to Mayo Clinic.