Overview
Rectal cancer
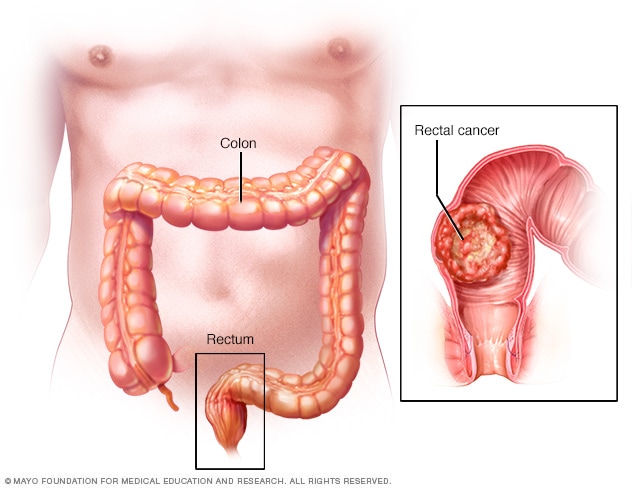
Rectal cancer
The rectum is the last several inches of the large intestine. Rectal cancer starts as a growth of cells in the rectum.
Rectal cancer is a kind of cancer that starts as a growth of cells in the rectum. The rectum is the last several inches of the large intestine. It starts at the end of the final segment of the colon and ends when it reaches the short, narrow passage known as the anus.
Cancer inside the rectum and cancer inside the colon are often referred to together as colorectal cancer.
While rectal and colon cancers are similar in many ways, their treatments are quite different. This is mainly because the rectum is barely separated from other organs and structures. It sits in a tight space that can make surgery to remove rectal cancer complex.
Rectal cancer treatment often involves surgery to remove the cancer. Other treatments may include chemotherapy, radiation or a combination of the two. Targeted therapy and immunotherapy also may be used.
Products & Services
Symptoms
Rectal cancer may not cause symptoms early on. Symptoms of rectal cancer usually happen when the disease is advanced.
Symptoms of rectal cancer in both men and women include:
- A change in bowel habits, such as diarrhea, constipation or a more frequent need to pass stool.
- A feeling that the bowel doesn't empty completely.
- Abdominal pain.
- Rectal bleeding, which may make stool look dark maroon or bright red in color.
- Narrow stool.
- Weight loss that happens without trying.
- Weakness or fatigue.
- A lump in the rectum, which may be found during a medical exam.
While rectal bleeding can be a sign of rectal cancer, it's often due to other causes, such as swollen veins in the rectum, called hemorrhoids. Generally, bleeding related to hemorrhoids is bright red and happens during or after bowel movements, while bleeding related to cancer may be dark or bright red and happen at any time. If you notice bleeding, it's important to see a healthcare professional and get checked because it's difficult to tell the difference between these two conditions.
When to see a doctor
Make an appointment with your doctor or other healthcare professional if you have any symptoms that worry you.
Causes
The exact cause of most rectal cancers isn't known.
Rectal cancer happens when cells in the rectum develop changes in their DNA. A cell's DNA holds the instructions that tell a cell what to do. In healthy cells, the DNA gives instructions to grow and multiply at a set rate. The instructions tell the cells to die at a set time. In cancer cells, the DNA changes give different instructions. The changes tell the cancer cells to make many more cells quickly. Cancer cells can keep living when healthy cells would die. This causes too many cells.
The cancer cells might form a mass called a tumor. The tumor can grow to invade and destroy healthy body tissue. In time, cancer cells can break away and spread to other parts of the body. When cancer spreads, it's called metastatic cancer. Although rectal cancer can spread to almost any organ, the liver and lungs are most commonly affected.
The majority of rectal cancers are adenocarcinomas. Adenocarcinoma is cancer that starts in gland cells, also called glandular cells. Gland cells are found all over the body, including in the rectum.
Risk factors
Factors that may increase the risk of rectal cancer are the same as those that increase the risk of colon cancer. Colorectal cancer risk factors include:
- A personal history of colorectal cancer or polyps. Your risk of colorectal cancer is higher if you've already had rectal cancer, colon cancer or adenomatous polyps.
- Black race. Black people in the United States have a greater risk of colorectal cancer than do people of other races.
- Diabetes. People with type 2 diabetes may have an increased risk of colorectal cancer.
- Drinking alcohol. Heavy drinking increases the risk of colorectal cancer.
- A diet low in vegetables. Colorectal cancer may be related to a diet low in vegetables and high in red meat.
- Family history of colorectal cancer. You're more likely to develop colorectal cancer if you have a parent, sibling or child with colon or rectal cancer.
- Inflammatory bowel disease. Chronic inflammatory diseases of the colon and rectum, such as ulcerative colitis and Crohn's disease, increase your risk of colorectal cancer.
- Inherited syndromes that increase colorectal cancer risk. In some families, DNA changes passed from parents to children may increase the risk of colorectal cancer. These changes are involved in only a small percentage of rectal cancers. Inherited syndromes may include familial adenomatous polyposis, also known as FAP, and Lynch syndrome. Genetic testing can detect these and other, rarer inherited colorectal cancer syndromes.
- Excess weight. People with obesity have an increased risk of colorectal cancer compared with people considered to be at a healthy weight.
- Older age. Colorectal cancer can be diagnosed at any age, but most people with this type of cancer are older than 50. The rates of colorectal cancer in people younger than 50 have been increasing, but healthcare professionals aren't sure why.
- Radiation therapy for previous cancer. Radiation therapy directed at the abdomen to treat previous cancers may increase the risk of colorectal cancer.
- Smoking. People who smoke may have an increased risk of colorectal cancer.
- Too little exercise. If you're inactive, you're more likely to develop colorectal cancer. Getting regular physical activity may reduce your risk of cancer.
Complications
Rectal cancer can lead to complications, including:
- Bleeding in the rectum. Rectal cancer often causes bleeding in the rectum. Sometimes the amount of blood is worrying, and treatment might be needed to stop it right away.
- Intestinal obstruction. Rectal cancer can grow to block the intestines. This prevents stool from leaving the body. Surgery to remove the cancer often relieves an obstruction. If you can't have surgery right away, you might need other treatments to ease the blockage.
- Intestinal perforation. Rectal cancer may cause a tear in the intestines. Perforation typically requires surgery.
Prevention
There's no sure way to prevent rectal cancer, but you can reduce your risk if you:
Ask about rectal cancer screening
Colorectal cancer screening reduces the risk of cancer by finding precancerous polyps in the colon and rectum that could turn into cancer. Ask your healthcare professional about when you should begin screening. Most medical organizations recommend starting screening around age 45. You may be screened earlier if you have risk factors for colorectal cancer.
Several screening options exist. Talk about your options with your healthcare professional. Together you can decide which tests are right for you.
Drink alcohol in moderation, if at all
If you choose to drink alcohol, do so in moderation. For healthy adults, that means up to one drink a day for women and up to two drinks a day for men.
Eat more fruits and vegetables
Choose a healthy diet with a variety of fruits and vegetables. Food sources of vitamins and nutrients are best. Avoid taking large doses of vitamins in pill form, as they may be harmful.
Exercise most days of the week
Aim for at least 30 minutes of exercise on most days of the week. If you haven't been active lately, ask your healthcare professional whether it's OK and start slowly.
Maintain a healthy weight
If your weight is healthy, work to maintain that weight. If you need to lose weight, ask a healthcare professional about healthy ways to lower your weight. Eat fewer calories and slowly increase the amount of exercise.
Stop smoking
Talk with your healthcare team about strategies and aids that can help you quit. Options include nicotine replacement products, medicines and support groups. If you've never smoked, don't start.
Sept. 12, 2025