Diagnosis
Currently, there isn't a specific test to diagnose Parkinson's disease. A diagnosis is made by a doctor trained in nervous system conditions, known as a neurologist. A diagnosis of Parkinson's is based on your medical history, a review of your symptoms, and a neurological and physical exam.
A member of your health care team may suggest a specific single-photon emission computerized tomography (SPECT) scan called a dopamine transporter (DAT) scan. Although this can help support the suspicion that you have Parkinson's disease, it is your symptoms and results of a neurological exam that ultimately determine the correct diagnosis. Most people do not require a DAT scan.
Your care team may order lab tests, such as blood tests, to rule out other conditions that may be causing your symptoms.
Imaging tests — such as an MRI, ultrasound of the brain and PET scans — also may be used to help rule out other disorders. Imaging tests aren't particularly helpful for diagnosing Parkinson's disease.
In addition to examining you, a member of your health care team may give you carbidopa-levodopa (Rytary, Sinemet, others), a Parkinson's disease medicine. You must be given a sufficient dose to show the benefit, as getting low doses for a day or two isn't reliable. Significant improvement with this medicine will often confirm your diagnosis of Parkinson's disease.
Sometimes it takes time to diagnose Parkinson's disease. Health care professionals may recommend regular follow-up appointments with neurologists trained in movement disorders to evaluate your condition and symptoms over time and diagnose Parkinson's disease.
However, a new test may be on the horizon. Researchers are studying a Parkinson's test that can detect the disease before symptoms begin. The test is called an alpha-synuclein seed amplification assay. In a 2023 study, researchers tested the spinal fluid of more than 1,000 people to look for clumps of the protein alpha-synuclein. Alpha-synuclein is found in Lewy bodies. It forms clumps that the body can't break down. The clumps spread and damage brain cells.
Alpha-synuclein clumps are a hallmark sign of Parkinson's disease. The test accurately identified people with Parkinson's disease 87.7% of the time. The test also was highly sensitive for detecting people at risk of Parkinson's disease.
This study of the alpha-synuclein seed amplification assay was the largest so far. Some researchers say the study may be a game changer for Parkinson's disease diagnosis, research and treatment trials. But larger studies are needed. There's hope among researchers that in the future, the test could be done using blood samples rather than spinal fluid.
Treatment
Parkinson's disease can't be cured, but medicines can help control the symptoms, often dramatically. In some more advanced cases, surgery may be advised.
Your health care team also may recommend lifestyle changes, especially ongoing aerobic exercise. In some cases, physical therapy that focuses on balance and stretching is important. A speech-language pathologist may help improve speech problems.
Medications
Medicines may help you manage problems with walking, movement and tremor. These medicines increase or substitute for dopamine.
People with Parkinson's disease have low levels of brain dopamine. However, dopamine can't be given directly because it can't enter the brain.
You may have significant improvement of your symptoms after beginning Parkinson's disease treatment. Over time, however, the benefits of medicines frequently diminish or become less consistent. You can usually still control your symptoms well.
Medicines your care team may prescribe include:
-
Carbidopa-levodopa (Rytary, Sinemet, Duopa, others). Levodopa, the most effective Parkinson's disease medicine, is a natural chemical that passes into the brain and is converted to dopamine.
Levodopa is combined with carbidopa (Lodosyn), which protects levodopa from early conversion to dopamine outside the brain. This prevents or lessens side effects such as nausea.
Side effects may include nausea or lightheadedness when you stand, called orthostatic hypotension.
After years, as your disease progresses, the benefit from levodopa may lessen, with a tendency to wax and wane, also called "wearing off."
Also, you may experience involuntary movements known as dyskinesia after taking higher doses of levodopa. Your care team may lessen your dose or adjust the times of your doses to control these effects.
Unless told otherwise by your health care team, carbidopa-levodopa is best taken on an empty stomach if you have advanced Parkinson's disease.
- Inhaled carbidopa-levodopa. Inbrija is a brand-name medicine delivering carbidopa-levodopa in an inhaled form. It may be helpful in managing symptoms that arise when medicines taken by mouth suddenly stop working during the day.
-
Carbidopa-levodopa infusion. Duopa is a brand-name medicine combining carbidopa and levodopa. However, it's administered through a feeding tube that delivers the medicine in a gel form directly to the small intestine.
Duopa is for patients with more-advanced Parkinson's who still respond to carbidopa-levodopa but who have a lot of fluctuations in their response. Because Duopa is continually infused, blood levels of the two medicines remain constant.
Placement of the tube requires a small surgical procedure. Risks associated with having the tube include the tube falling out or infections at the infusion site.
-
Dopamine agonists. Unlike levodopa, dopamine agonists don't change into dopamine. Instead, they mimic dopamine effects in the brain.
Dopamine agonists aren't as effective as levodopa in treating symptoms. However, they last longer and may be used with levodopa to smooth the sometimes off-and-on effect of levodopa.
Dopamine agonists include pramipexole (Mirapex ER) and rotigotine (Neupro), which is given as a patch. Apomorphine (Apokyn) is a short-acting dopamine agonist shot used for quick relief.
Some of the side effects of dopamine agonists are like the side effects of carbidopa-levodopa. But they also can include hallucinations, sleepiness and compulsive behaviors such as hypersexuality, gambling and eating. If you're taking these medicines and you behave in a way that's out of character for you, talk to your health care team.
-
Monoamine oxidase B (MAO B) inhibitors. These medicines include selegiline (Zelapar), rasagiline (Azilect) and safinamide (Xadago). They help prevent the breakdown of brain dopamine by inhibiting the brain enzyme monoamine oxidase B (MAO B). This enzyme breaks down brain dopamine. Selegiline given with levodopa may help prevent wearing off.
Side effects of MAO B inhibitors may include headaches, nausea or insomnia. When added to carbidopa-levodopa, these medicines increase the risk of hallucinations.
These medicines are not often used in combination with most antidepressants or certain pain medicines due to potentially serious but rare reactions. Check with your health care team before taking any additional medicines with an MAO B inhibitor.
-
Catechol O-methyltransferase (COMT) inhibitors. Entacapone (Comtan) and opicapone (Ongentys) are the primary medicines from this class. This medicine mildly prolongs the effect of levodopa therapy by blocking an enzyme that breaks down dopamine.
Side effects, including an increased risk of involuntary movements called dyskinesia, mainly result from an enhanced levodopa effect. Other side effects include diarrhea, nausea or vomiting.
Tolcapone (Tasmar) is another COMT inhibitor that is rarely prescribed due to a risk of serious liver damage and liver failure.
-
Anticholinergics. These medicines were used for many years to help control the tremor associated with Parkinson's disease. Several anticholinergic medicines are available, including benztropine (Cogentin) or trihexyphenidyl.
However, their modest benefits are often offset by side effects such as impaired memory, confusion, hallucinations, constipation, dry mouth and impaired urination.
-
Amantadine. Health care professionals may prescribe amantadine (Gocovri) alone to provide short-term relief of symptoms of mild, early-stage Parkinson's disease. It also may be given with carbidopa-levodopa therapy during the later stages of Parkinson's disease to control involuntary movements called dyskinesia induced by carbidopa-levodopa.
Side effects may include a change in skin color, ankle swelling or hallucinations.
- Adenosine receptor antagonists (A2A receptor antagonists). These drugs target areas in the brain that regulate the response to dopamine and allow more dopamine to be released. Istradefylline (Nourianz) is one of the A2A antagonist drugs.
- Nuplazid (Pimavanserin). This drug is used to treat hallucinations and delusions that can occur with Parkinson's disease. Experts aren't sure how it works.
Surgical procedures
Deep brain stimulation
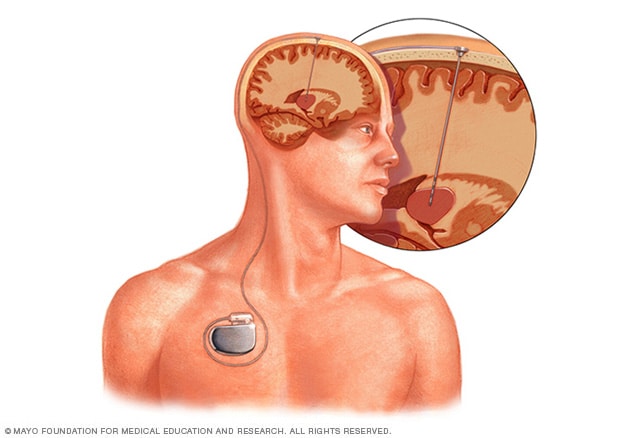
Deep brain stimulation
Deep brain stimulation involves implanting an electrode deep within the brain. The amount of stimulation delivered by the electrode is controlled by a pacemaker-like device placed under the skin in the chest. A wire that travels under the skin connects the device to the electrode.
-
Deep brain stimulation. In deep brain stimulation (DBS), surgeons implant electrodes into a specific part of the brain. The electrodes are connected to a generator implanted in the chest near the collarbone. The generator sends electrical pulses to the brain and may reduce Parkinson's disease symptoms.
Your health care team may adjust your settings as necessary to treat your condition. Surgery involves risks, including infections, stroke or brain hemorrhage. Some people experience problems with the DBS system or have complications due to stimulation. A member of your health care team may need to adjust or replace some parts of the system.
Deep brain stimulation is most often offered to people with advanced Parkinson's disease who have unstable responses to levodopa. DBS can stabilize medicine fluctuations, reduce or halt involuntary movements called dyskinesia, reduce tremor, reduce rigidity, and improve movements.
DBS is effective for controlling changing responses to levodopa or for controlling dyskinesia that doesn't improve with medicine adjustments.
However, DBS isn't helpful for problems that don't respond to levodopa therapy apart from tremor. Tremor may be controlled by DBS even if the tremor isn't very responsive to levodopa.
Although DBS may provide sustained benefit for Parkinson's symptoms, it doesn't keep Parkinson's disease from progressing.
Advanced treatments
MRI-guided focused ultrasound (MRgFUS) is a minimally invasive treatment that has helped some people with Parkinson's disease manage tremors. Ultrasound is guided by an MRI to the area in the brain where the tremors start. The ultrasound waves are at a very high temperature and burn areas that are contributing to the tremors.
More Information
Clinical trials
Explore Mayo Clinic studies testing new treatments, interventions and tests as a means to prevent, detect, treat or manage this condition.
Lifestyle and home remedies
You'll need to work closely with your health care team to find a Parkinson's treatment plan that offers you the greatest relief from symptoms with the fewest side effects. Certain medicines can make your symptoms worse, so please discuss with your care team any medicines you currently take.
Certain lifestyle changes also may help make living with Parkinson's disease easier.
Healthy eating
While no food or combination of foods has been proved to help in Parkinson's disease, some foods may help ease some of the symptoms. For example, eating foods high in fiber and drinking plenty of fluids can help prevent constipation that is common in Parkinson's disease.
A balanced diet also provides nutrients, such as omega-3 fatty acids, that might be beneficial for people with Parkinson's disease.
Exercise
Exercising may increase your muscle strength, flexibility and balance. Exercise also can improve your well-being and reduce depression or anxiety.
Your health care team may suggest that you work with a physical therapist to learn an exercise program that works for you. You also may try exercises such as walking, swimming, gardening, dancing, water aerobics or stretching.
Parkinson's disease can disturb your sense of balance, making it difficult to walk with your usual gait. Exercise may improve your balance. These suggestions also may help:
- Try not to move too quickly.
- Aim for your heel to strike the floor first when you're walking.
- If you notice yourself shuffling, stop and check your posture. It's best to stand up straight.
- Look in front of you, not directly down, while walking.
Avoiding falls
In the later stages of the disease, you may fall more easily. In fact, you may be thrown off balance by just a small push or bump. The following suggestions may help:
- Make a U-turn instead of pivoting your body over your feet.
- Distribute your weight evenly between both feet, and don't lean.
- Avoid carrying things while you walk.
- Avoid walking backward.
Daily living activities
Daily living activities — such as dressing, eating, bathing and writing — can be difficult for people with Parkinson's disease. An occupational therapist can show you techniques that make daily life easier.
If you are having trouble talking, a speech therapist may be able to help. Many people with Parkinson's disease have speech difficulties such as a slow, weak voice, trouble with consonants, slurred speech, a low voice that has a monotone with little expression, and inappropriate silences. A speech therapist may be able to help with these problems.
Alternative medicine
Supportive therapies can help ease some of the symptoms and complications of Parkinson's disease, such as pain, fatigue and depression. When performed in combination with your treatments, these therapies might improve your quality of life:
- Massage. Massage therapy can reduce muscle tension and promote relaxation. This therapy, however, is rarely covered by health insurance.
-
Tai chi. An ancient form of Chinese exercise, tai chi uses slow, flowing motions that may improve flexibility, balance and muscle strength. Tai chi also may help prevent falls. Several forms of tai chi are tailored for people of any age or physical condition.
A study showed that tai chi may improve the balance of people with mild to moderate Parkinson's disease more than stretching and resistance training do.
- Yoga. In yoga, gentle stretching movements and poses may increase your flexibility and balance. You may modify most poses to fit your physical abilities.
- Alexander technique. This technique — which focuses on muscle posture, balance and thinking about how you use muscles — may reduce muscle tension and pain.
- Meditation. In meditation, you quietly reflect and focus your mind on an idea or image. Meditation may reduce stress and pain and improve your sense of well-being.
- Pet therapy. Having a dog or cat may increase your flexibility and movement and improve your emotional health.
- Relaxation techniques. These practices help lower your blood pressure, reduce your heart rate and improve muscle tone.
Coping and support
Living with any chronic illness can be difficult, and it's not uncommon to feel angry, depressed or discouraged at times. Parkinson's disease can be profoundly frustrating as walking, talking and even eating become more difficult and time-consuming.
Depression is common in people with Parkinson's disease. But antidepressant medicines can help ease the symptoms of depression, so talk with your health care team if you're feeling persistently sad or hopeless.
Although friends and family can be your best allies, the understanding of people who know what you're going through can be especially helpful. Support groups aren't for everyone. However, for many people with Parkinson's disease and their families, a support group can be a good resource for practical information about Parkinson's disease.
Also, groups offer a place for you to find people who are going through similar situations and can support you.
Trying to maintain some of your usual activities may be helpful. Aim to do as many things as possible that you could do before the onset of Parkinson's disease. Focus on the present and try to maintain a positive attitude.
To learn about support groups in your community, talk to your health care team, a Parkinson's disease social worker or a local public health nurse. Or contact the Parkinson's Foundation or the American Parkinson Disease Association.
You and your family also may benefit from talking to a mental health professional, such as a psychologist or social worker trained in working with people who have chronic conditions.
Preparing for your appointment
You're likely to first see a health care professional. You may then be referred to a doctor trained in nervous system disorders, called a neurologist.
Because there's often a lot to discuss, it's a good idea to prepare for your appointment. Here's some information to help you get ready for your appointment.
What you can do
- Write down any symptoms you're experiencing, including any that may seem unrelated to the reason for which you scheduled the appointment.
- Write down key personal information, including any major stresses or recent life changes.
- Make a list of all medicines, vitamins and supplements that you're taking.
- Ask a family member or friend to come with you, if possible. Sometimes it can be difficult to remember all the information provided to you during an appointment. Someone who goes with you may remember something that you missed or forgot.
- Write down questions to ask during your appointment.
Your time with your care team is limited, so preparing a list of questions ahead of time will help you make the most of your time together. For Parkinson's disease, some basic questions to ask include:
- What's the most likely cause of my symptoms?
- Are there other possible causes?
- What kinds of tests do I need? Do these tests require any special preparation?
- How does Parkinson's disease usually progress?
- Will I eventually need long-term care?
- What treatments are available, and which do you recommend for me?
- What types of side effects can I expect from treatment?
- If the treatment doesn't work or stops working, do I have additional options?
- I have other health conditions. How can I best manage these conditions together?
- Are there any brochures or other printed material that I can take home with me? What websites do you recommend?
In addition to the questions that you've prepared to ask your care team, don't hesitate to ask questions that occur to you during your appointment.
What to expect from your doctor
Your health care team is likely to ask you a several questions. Being ready to answer them may reserve time to go over any points you want to spend more time on. You may be asked:
- When did you first begin experiencing symptoms?
- Do you have symptoms all the time, or do they come and go?
- Does anything seem to improve your symptoms?
- Does anything seem to make your symptoms worse?