Feb. 09, 2019
Primary sclerosing cholangitis (PSC) is a chronic, idiopathic biliary tract disease characterized by inflammation, fibrosis and strictures that can progress to cirrhosis and end-stage liver disease. PSC is progressive and associated with a significantly elevated risk of cancers of the liver, gallbladder, bile ducts and colon. The length of time it takes for the disease to progress can vary. In some individuals, PSC progresses rapidly after diagnosis. Others can go decades without significant progression or symptoms.
The cause of PSC is unclear. A combination of genetic predisposition and immune system factors could be involved. The majority of patients with PSC are male, and nearly 80 percent also have inflammatory bowel disease (IBD).
About 50 percent of patients with PSC have no clinical symptoms, and diagnosis occurs after the discovery of elevated liver enzymes during routine bloodwork. Symptoms can include pruritus, right upper quadrant abdominal pain and acute bacterial cholangitis.
Mayo Clinic specialists in gastroenterology and hepatology see a very large cohort of patients with PSC and employ highly specialized endoscopic practices to diagnose and manage this disease and its complications.
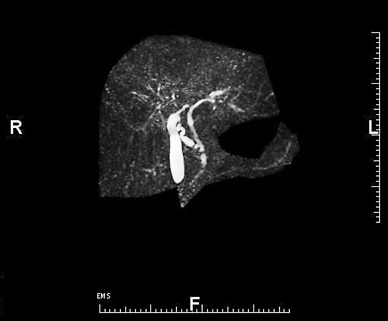
MRCP helps confirm liver and biliary tract abnormalities
MRCP helps confirm liver and biliary tract abnormalities
High-quality cross-sectional cholangiographic imaging, such as this magnetic resonance cholangiopancreatography (MRCP), can help confirm the presence of liver and biliary tract abnormalities associated with primary sclerosing cholangitis.
ERCP showing strictures in the hepatic biliary system

ERCP showing strictures in the hepatic biliary system
Corresponding endoscopic retrograde cholangiopancreatography (ERCP) cholangiogram shows strictures in the hepatic biliary system.
High-quality cross-sectional cholangiographic imaging can help confirm the presence of liver and biliary tract abnormalities associated with PSC. Magnetic resonance cholangiopancreatography (MRCP) provides indirect visualization of the bile ducts and the presence of inflammatory strictures, fibrotic biliary tree changes and bile duct dilation, all in a noninvasive and essentially risk-free platform.
"In most individuals with PSC, MRCP will reveal diffuse biliary changes, including multifocal stricturing within the intrahepatic and/or extrahepatic bile ducts, accompanied by upstream dilation," explains M. Edwyn Harrison, M.D., a gastroenterologist at Mayo Clinic's campus in Arizona. "About 20 percent of individuals with PSC will present with biliary changes limited to the intrahepatic ducts," says Dr. Harrison.
The use of endoscopic retrograde cholangiopancreatography (ERCP) as a diagnostic tool has declined now that MRCP is available. "Therapeutic ERCP is appropriate for use in patients who develop pain with abrupt elevations in bilirubin, acute cholangitis or progressive dominant strictures on MRCP," explains Dr. Harrison.
Dominant strictures typically occur in about half of patients with PSC and can lead to biliary obstruction. "In these patients, therapeutic ERCP is useful for dilation and stent placement in PSC-induced dominant strictures," says John A. Martin, M.D., a gastroenterologist at Mayo Clinic's campus in Rochester, Minnesota. "This would include strictures with a diameter of 1.5 mm in the common bile duct or 1 mm in the intrahepatic duct," says Dr. Martin.
Drs. Harrison and Martin also caution that because complications associated with ERCP include pancreatitis and cholangitis, this procedure should be performed by experienced endoscopists in high-volume centers.
Cancer surveillance
Because malignancy causes substantial morbidity and mortality in individuals with PSC, heightened cancer surveillance is recommended. Mayo Clinic endoscopists employ specialized screening tools and evidence-based protocols to reduce the disease burden in this population.
Cholangiocarcinoma
Individuals with PSC have a lifetime risk of cholangiocarcinoma (CCA) ranging from 5 to 20 percent. Current guidelines recommend a serial ultrasound or an MRI/MRCP and CA 19-9 to screen for CCA every six to 12 months.
When used alone, imaging studies don't provide a high degree of sensitivity and specificity, so Mayo Clinic endoscopists also commonly employ forceps biopsies and fluorescence in situ hybridization (FISH) and cholangioscopy during ERCP to screen for dysplasia or CCA. FISH uses fluorescently labeled DNA probes to identify the presence of chromosomal abnormalities in bile duct cells to enhance diagnostic sensitivity.
"In patients with a dominant stricture identified during imaging, we consider performing ERCP with brush cytology, forceps biopsies and FISH to confirm or rule out the presence of dysplasia or cholangiocarcinoma," says Dr. Martin.
Authors of a study published in Therapeutic Advances in Gastroenterology in 2015 concluded that this triple-modality approach offers improved sensitivity and specificity for the diagnosis of CCA (82 percent) when compared with conventional brush cytology alone or other single-modality testing (27 to 59 percent).
Researchers are also investigating additional markers for CCA with the goal of developing a more sensitive diagnostic screening tool. Some experts believe that specific serum microRNAs, a class of noncoding RNAs involved in gene regulation, could serve as diagnostic and prognostic biomarkers for both PSC and CCA.
Gallbladder cancer
Individuals with PSC have a lifetime risk of gallbladder cancer of approximately 2 percent. Mayo staff note that annual imaging with MRCP to screen for the development of CCA is also useful to screen for gallbladder cancer.
Colorectal cancer
Individuals with PSC and concomitant IBD are at increased risk of colorectal carcinoma. Mayo Clinic IBD specialists recommend surveillance colonoscopy annually to screen for any precancerous or cancerous colon lesions. Chromoendoscopy is often considered in these patients to increase the sensitivity for detecting premalignant dysplasia, especially in patients who have previously had indefinite dysplasia.
Liver transplantation
About 40 percent of individuals with PSC will eventually require a liver transplant. Transplantation can be considered for individuals who develop evidence of decompensated cirrhosis and those with PSC-related complications, including refractory pruritus or recurrent cholangitis.
In the past, a diagnosis of unresectable hilar CCA was considered a contraindication for liver transplantation due to frequent recurrence and poor long-term survival. In 1993, Mayo Clinic developed a novel therapeutic protocol combining neoadjuvant chemoradiation and orthotopic liver transplantation to treat patients with unresectable hilar CCA or CCA arising in the setting of PSC.
A report authored by Mayo Clinic transplant specialists and published in HPB in 2008 demonstrated that the combination of neoadjuvant therapy, operative staging to rule out regional metastases and liver transplantation has achieved remarkable success for selected patients with early-stage hilar CCA.
"Our liver transplant program remains one of the few centers nationwide that performs transplants on these patients," notes co-author Gregory J. Gores, M.D., a transplant hepatologist at Mayo Clinic's campus in Rochester, Minnesota.
Summary
Advanced endoscopic techniques performed by experienced endoscopists can enhance the diagnosis and management of PSC and aid in surveillance for hepatobiliary malignancy. When combined with neoadjuvant chemoradiation, orthotopic liver transplantation can be used to treat patients with unresectable CCA associated with PSC.
For more information
Nanda A, et al. Triple modality testing by endoscopic retrograde cholangiopancreatography for the diagnosis of cholangiocarcinoma. Therapeutic Advances in Gastroenterology. 2015;8:56.
Rosen CB, et al. Surgery for cholangiocarcinoma: The role of liver transplantation. HPB. 2008;10:186.