April 13, 2019
In this Q and A, three experienced therapeutic endoscopists from Mayo Clinic answer questions about the role of endoscopic submucosal dissection (ESD) in treating lesions within the gastrointestinal tract. Norio Fukami, M.D., from Mayo Clinic's campus in Scottsdale, Arizona; Michael B. Wallace, M.D., from Mayo Clinic's campus in Jacksonville, Florida; and Louis M. Wong Kee Song, M.D., from Mayo Clinic's campus in Rochester, Minnesota, share best practices and updates about the role of ESD within the United States.
What are the indications for ESD for treatment of early gastric cancers?
ESD has enabled en bloc resection of lesions that are too large for endoscopic mucosal resection (EMR) and those that are suspected superficial malignancies. An AGA Institute Clinical Practice Update published in Clinical Gastroenterology and Hepatology in 2019 outlines several best practices for ESD. Peter V. Draganov, M.D., Dr. Fukami and co-authors note that historically, absolute indications for endoscopic resection have included mucosal cancers ≤ 2 cm that are moderately and well-differentiated and nonulcerated. The authors also state that ESD has enabled the expansion of endoscopic resection criteria, so it may also be appropriate to include: moderately and well-differentiated superficial gastric cancers that are larger than 2 cm, lesions ≤ 3 cm with ulceration or those that contain early submucosal invasion, and poorly differentiated superficial cancers ≤ 2 cm. However, performing ESD for these expanded indications can lead to including patients who have an elevated risk of lymph node metastasis. So success in completing safe ESD and an analysis of post-resection pathological findings are extremely important to consider when assessing the need for additional oncologic therapy.
Is ESD appropriate for patients with Barretts esophagus-related neoplasms?
Although EMR is performed in most cases, ESD may be considered for select patients with Barrett's esophagus. Experienced endoscopists are more likely to use this approach in patients with suspected superficial cancers (T1a and early T1b lesions) that are larger than 10 to 15 mm, and those with poor lifting. The AGA update states that ESD may be considered for lesions that have a large or bulky area of nodularity, lesions where superficial submucosal invasion is suspected, and for those with evidence of recurrent dysplasia, invasive carcinoma with positive margins, equivocal pre-procedural histology or intramucosal carcinoma.
What role can ESD play in treating esophageal squamous cell carcinoma (ESCC)?
According to the AGA update, ESD is the primary modality for treating ESCC confined to the superficial esophageal mucosa. The authors also note that alternative or additional therapy should be considered for lesions with pathological evidence of submucosal invasion, due to increased risk of lymph node metastasis. Large uninterrupted specimen removed by ESD technique would facilitate the pathological evaluation of the lesion to determine tumor staging and a risk of metastasis. The European Society of Gastrointestinal Endoscopy (ESGE) guideline published in Endoscopy in 2015 recommends en bloc ESD resection instead of EMR for ESCC lesions 10 mm or larger.
Data from large trials with head-to-head comparisons between ESD and esophagectomy using a validated assessment tool in patients with ESCC still remain scarce.
In an article published in Gastrointestinal Endoscopy in 2018, Yang Won Min, M.D., Ph.D., and co-authors shared the results from a retrospective, single-center analysis comparing outcomes between two groups of patients. One group underwent ESD for ESCC. The other underwent esophagectomy, but the patients were later deemed candidates for ESD by a retrospective review of images, as determined by the study protocol. Both groups received long-term follow-up with serial upper endoscopy and chest CT at set intervals until five years after intervention. Patients in the ESD group had outcomes that were similar to those in the group that underwent surgical therapy. The ESD group also had lower adverse event occurrences, even though metachronous lesions were more frequent in this group.
In an editorial published in Gastrointestinal Endoscopy in 2018 and commenting on this study, Dr. Fukami and co-author Tiffany Y. Chua, M.D., note that the study results suggest that ESD can serve as a first line treatment for superficial ESCC when endoscopic features do not indicate submucosal invasion and when there is no clinical evidence of metastasis.
What has recent research shown about the use of ESD for colorectal lesions?
Advanced endoscopic techniques should be considered for complex colorectal lesions without signs of deep submucosal invasion or advanced cancer. ESGE guideline notes that ESD is generally appropriate for colonic lesions larger than 2 cm that are suspected invasive cancer with limited (shallow) invasion depth, all rectal lesions larger than 2 cm that are nongranular, and those larger than 3 cm that are granular or mixed. The AGA update also notes that neoplasms containing dysplasia confined to the mucosa have no risk of lymph node metastasis, and therefore endoscopic resection should be the primary mode of therapy. ESD should be considered for large lesions or those with concerning features for superficial colorectal cancer.
What challenges do larger or more-complex colorectal lesions pose?
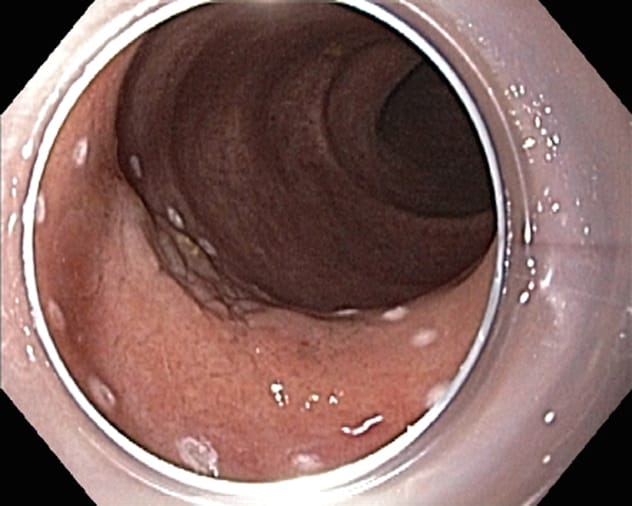 ورم كبير مثبت من خلال خزعة وسطحي مميز بنقاط متخثرة
ورم كبير مثبت من خلال خزعة وسطحي مميز بنقاط متخثرة
 تشريح النسيج تحت المخاطي بالتنظير الداخلي
تشريح النسيج تحت المخاطي بالتنظير الداخلي
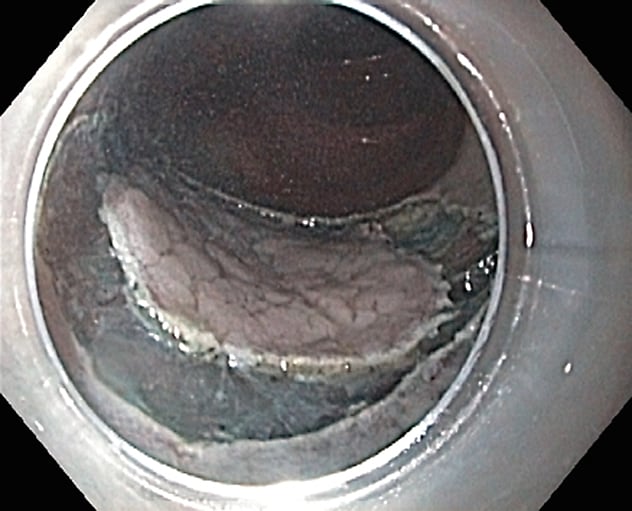
 عيب تشريحي تحت المخاطية بعد جراحة المناظير
عيب تشريحي تحت المخاطية بعد جراحة المناظير
Experienced endoscopists agree that patients with lesions larger than 2 cm and complex colorectal polyps should be referred to a high-volume, specialized center for endoscopic removal using EMR or ESD. Piecemeal removal of larger lesions is associated with an increased rate of recurrence up to 20 percent, and an incomplete first attempt is associated with an increased rate of failure of future endoscopic therapy. ESD can facilitate en bloc resection and reduce recurrence rates in patients with these larger, more-complex lesions.
What do ESD practitioners need to know about closure devices?
The AGA update notes that familiarity with closure devices, including clips and endoscopic suturing, is important. Available data show that both approaches are effective in managing intraprocedural perforation.
How can clinicians acquire ESD training in the United States?
While there is no standardized approach to ESD training within the U.S., it is still possible to achieve a high level of competency in this procedure. Self-guided study, practice on explant and animated models, and training courses offered by Mayo Clinic and other high-volume, advanced endoscopy centers and GI societies can provide the needed exposure and opportunities for skill development.
Are there new technologies that will make ESD simpler?
One of the major limitations of ESD is the very long time needed to complete the procedure. ESD typically requires two to three hours, which is nearly two times longer than EMR and four to six times longer than the time required for diagnostic colonoscopy. Several new devices that allow traction and countertraction, as well as electrosurgical knives with integrated water jets to lift and cut simultaneously, have recently been introduced and are under study.
For more information
Draganov PV, et al. AGA Institute Clinical Practice Update: Endoscopic Submucosal Dissection in the United States. Clinical Gastroenterology and Hepatology. 2019;17:16.
Pimentel-Nunes P, et al. Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2015;47:829.
Min YW, et al. Comparison of endoscopic submucosal dissection and surgery for superficial esophageal squamous cell carcinoma: A propensity score-matched analysis. Gastrointestinal Endoscopy. 2018;88:624.
Chua T, et al. Upfront endoscopic submucosal dissection for superficial squamous cell carcinoma is superior to upfront surgical therapy. Gastrointestinal Endoscopy. 2018;88:634.