Sept. 05, 2012
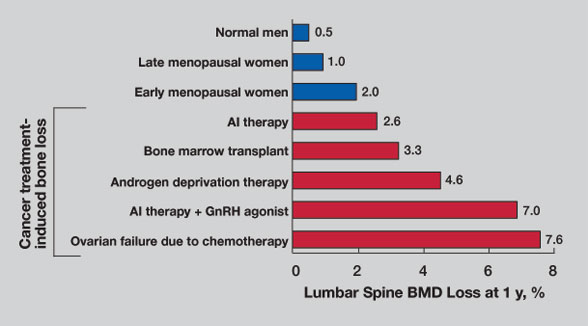
Annualized bone mineral density losses
Annualized bone mineral density losses
Comparison of annualized lumbar spine bone mineral density (BMD) losses associated with normal aging (top; blue bars) to BMD losses associated with different cancer therapies (bottom; red bars). AI indicates aromatase inhibitor; GnRH, gonadotropin-releasing hormone. Adapted from Postgraduate Institute for Medicine and Interlink Healthcare Communications, joint sponsors of the CME Lecture Series titled Skeletal Complications Across the Cancer Continuum Slide/Lecture Kit, June 2005. Used with permission from Postgraduate Institute for Medicine (http://www.pimed.com/index.asp).
Nearly all cancers can have clinically significant negative effects on the skeleton. Matthew T. Drake, M.D., Ph.D., of the Division of Endocrinology, Diabetes, Metabolism and Nutrition at Mayo Clinic in Rochester, Minn., says: "Cancer is a major risk factor for both generalized and local bone loss, with bone loss in patients with cancer substantially greater than in the general population.
"Cancer-associated bone loss is due to the direct effects of cancer cells and the effects of therapies used in cancer treatment, including chemotherapeutics, corticosteroids, aromatase inhibitors and androgen-deprivation therapy (ADT). The skeleton is also the most common site of metastatic disease, because cancer cells growing within bone induce osteoblasts and osteoclasts to produce factors that stimulate further cancer growth. Accordingly, skeletal effects have become increasingly important because of improved oncologic treatments that have enhanced both patient survival and longevity."
Breast cancer
Morbidity due to bone disease in patients with breast cancer can have a major impact on patient quality of life because of the often long clinical course. Bone-related complications in women with breast cancer include:
- Hypercalcemia
- Fractures
- Need for irradiation or surgery
- Spinal cord compression
Placebo-controlled trials have shown that in the absence of bone-protective therapies, patients have roughly 2.2 to 4.0 skeleton-related events annually.
Dr. Drake explains: "Although estrogen plays a central role in bone homeostasis, hormonal therapy-based treatment regimens to effect estrogen action at the estrogen receptor (ER) are frequently used. Tamoxifen is an ER antagonist in breast tissue that is often used for patients whose breast cancer is ER-positive, and as prophylaxis in patients at high risk of breast cancer. Tamoxifen may lead to bone loss in premenopausal women.
"By comparison, in postmenopausal women, tamoxifen can act as an ER agonist in bone and increase bone mass. However, neither tamoxifen nor raloxifene appear to reduce fracture incidence in postmenopausal women with breast cancer. Aromatase inhibitors decrease cancer recurrence and improve disease-free survival compared to tamoxifen. These inhibitors also result in significant bone loss and increased fracture incidence, as demonstrated in both the Arimidex, Tamoxifen, Alone or in Combination (ATAC) and Breast International Group 1-98 trials.
"Upfront, vs. delayed, zoledronate therapy improved bone mineral density (BMD) in postmenopausal women receiving adjuvant aromatase inhibitor therapy in the Zoledronic Acid-Letrozole Adjuvant Synergy Trial (ZFAST). More recently, denosumab was shown to increase the time to first skeleton-related event in patients with breast cancer."
Prostate cancer
ADT is often used for palliation in patients with prostate cancer. It induces clinically significant bone loss, likely because of the decreased availability of testosterone for conversion to estradiol. ADT also increases fracture risk. Yet, despite these profound skeletal effects, the majority of prostate cancer patients continue to be inadequately treated for their bone loss.
Dr. Drake says: "In prostate cancer, zoledronate is the best-studied bisphosphonate. Zoledronate has been shown to decrease bone loss and fracture risk, as well as to reduce bone loss induced by gonadotropin-releasing hormone agonist. More recently, denosumab was shown to increase BMD in patients with prostate cancer receiving ADT and to prolong the time to first skeleton-related event relative to zoledronate."
Monoclonal gammopathies
Myeloma is the second most common hematologic cancer, accounting for 10 percent of all hematologic cancers. Patients have both generalized bone loss and focal osteolytic lesions. Nearly two-thirds of patients with myeloma have bone pain at presentation, and fracture rates are sixteenfold relative to the general population in the year preceding diagnosis. Even with disease remission, skeletal lesions rarely heal.
Dr. Drake highlights: "Both pamidronate and zoledronate are approved by the U.S. Food and Drug Administration for the treatment of myeloma-related bone disease and have been shown in placebo-controlled trials to reduce hypercalcemia, bone pain and fracture incidence.
"Importantly, patients with monoclonal gammopathy of undetermined significance (MGUS), a common premalignant condition with an approximately 1 percent annual risk of progression to myeloma, have substantially increased fracture rates. We recently demonstrated that, relative to matched control subjects, patients with MGUS have decreases in both cortical and trabecular thickness, as well as increases in circulating cytokines known to increase osteoclast activity and suppress osteoblast activity. Together, these findings may provide insight into the increased fracture incidence seen in MGUS."
Potential complications of pharmacologic therapies
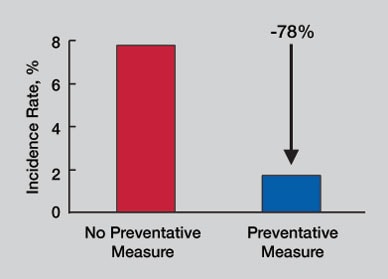
Effect of preventive dental measures
Effect of preventive dental measures
These measures can substantially reduce (in this case, reduced by 78 percent) the incidence of osteonecrosis of the jaw in cancer patients receiving high-dose intravenous bisphosphonate therapy. Adapted from Ripamonti CI, et al. Decreased occurrence of osteonecrosis of the jaw after implementation of dental preventive measures in solid tumour patients with bone metastases treated with bisphosphonates. The experience of the National Cancer Institute of Milan (http://annonc.oxfordjournals.org/content/20/1/137.full?sid=8e7d994b-4eea-466d-a80f-adffba47f208). Annals of Oncology.2009;20:137-45. Used with permission.
Osteonecrosis of the jaw (ONJ) is now a well-recognized potential complication of anti-resorptive therapy. Risk factors for ONJ include:
- Invasive dental procedures
- Poor oral hygiene
- Prolonged anti-resorptive therapy
Dr. Drake says: "Initial results suggest that rates of ONJ are comparable between zoledronate and denosumab in patients with cancer. Preventive dental measures in high-risk patients can substantially reduce risks; conservative management with oral rinses, pain control, antibiotics and limited surgical intervention will lead to healing in most cases. Although now recognized as very uncommon events in osteoporosis patients, atypical femoral fractures are currently limited to rare case reports in the oncologic literature. Hypocalcemia is most common in patients receiving intravenous bisphosphonate therapy; rates appear similar between zoledronate and denosumab. Risk can be limited by optimizing the intake and levels of calcium, vitamin D and magnesium."
Other factors for optimizing skeletal health
In addition to pharmacologic interventions, conservative measures are extremely important for patients with cancer in limiting fracture risk. Dr. Drake advises that conservative measures include:
- Counseling about high-risk activities (falls and heavy lifting)
- The introduction of appropriately supervised physical therapy for muscle strengthening to limit fall risks
- Ensuring adequate calcium and vitamin D intake after resolution of any existing hypercalcemia
"Finally, it is important to recognize that patients with cancer are often at increased fall risk due to the use of analgesics and sedatives. In conclusion, careful monitoring of bone health must be an essential component of any cancer treatment plan," says Dr. Drake.